Who knew the history of trying and testing for pregnancy would be so intertwined with maritime history? When I started my project, I never expected to be contemplating a visit to the National Maritime Museum archives in Greenwich, looking for ships, routes and cargoes. In my last post I talked about ships and now there are others coming up, too; it turns out I need to know a lot lot more about ships and sailors.
At the moment I’m thinking about the sixteenth century, exploring the story of Mary Tudor’s two false pregnancies (1554 and 1557). This has immersed me in texts and interests from the immediate aftermath of her death, and the reign of another childless Tudor queen, Elizabeth I. I have been looking at different writings from historians and poets, medical writers and others. Any historians of medicine reading this will know that health was intimately tied up with environmental factors in the medieval and Renaissance past and, not least, the wind. Wind was thought to blow through people connecting them up with the larger world, cosmos and elements.
Detail of Zephyrus and Chloris, Botticelli’s Birth of Venus (1480s).
Wind also had a special association with conception. Foetuses were thought to be ensouled at quickening through inspiration: they were literally breathed into life. Zephyrus, the west wind, from classical myth was thought to cause or contribute to the ripening of nature in the spring, at a historical moment when humans were not excepted from seasonal rhythms. You may know the opening to the Canterbury Tales which famously credits Zephyrus with pricking the spirits of little birds and simultaneously stirring longing for pilgrimage in people with all the opportunities pilgrimage offers for pleasure, for company, for reproduction of all kinds. Yet wind wasn’t only breath and life, it could also be flatulence and vacancy. Windy dropsy or windy tympany was the most common condition to be mistaken for pregnancy, because it swelled the stomach, just like in a pregnancy. Thinking about wind in relation to pregnancy enabled an agnosticism at a time when early pregnancy was often difficult to diagnose.
Wind rose from Cecco d’Ascoli, ‘L’Acerba’ (1521).
Entangled in the question of the wind and how responsible it was for royal reproductive disappointment and, by extension, England’s growing succession crisis, is an interest in the wind in relation to England’s maritime fortunes. To that end, I have recently been looking at the way that the winds are presented on maps, as individual personified beings at different points of the compass, drawn on maps as elaborate wind roses. ‘Winds’, writes Henry Peacham in The Gentlemans Exercise, ‘must be drawn with puffed and blowne cheekes,’ (rounded out but hollow shapes, like the abdomen distended by dropsy). In some ways there was less of a distinction than we might expect between wind roses and the representation of compasses. At a time when ships were sailing ships, winds were routes and, whilst land maps in the Middle Ages weren’t much used for getting around, sea charts or portolans certainly were.[1] Maps’ rhumb lines were the roads over which ships traveled and they lined up with the points of the compass, which also indicated the direction of different winds.
Medal commemorating the defeat of the Spanish Armada (1588), National Maritime Museum, London.
The wind was, of course, central to English maritime survival in the Anglo-Spanish wars of the late sixteenth centuries, which pitted Mary’s husband, Philip II of Spain, against Elizabeth, his one-time sister-in-law. Indeed, the Armada was defeated more by the wind than Elizabeth’s navy. Commemorative medals were made which celebrated this divine intervention in human affairs; ‘he blew’, the Latin caption read, citing the Biblical book of Job, ‘and they were scattered’. The Anglo-Spanish wars were also triangulated with America in an age of competitive colonial expansion, a project to which wind was, of course, absolutely crucial.
Detail of textiles in Armada portrait
Armada Portrait of Elizabeth I, one of three painted to commemorate the defeat of the Spanish Armada (1588). Royal Museums Greenwich.
I’m finding that these winds out at sea were the same ones, and sometimes discussed in the same breath as those that were implicated in Mary’s false pregnancies, and perhaps Elizabeth’s childlessness, too. So now I am looking at some of the very famous paintings and keep seeing wind roses everywhere. There are certainly a lot of rounded out forms – the globe, etc. in this much-discussed Armada portrait; and what do you think of the designs in the background textiles here, particularly on the right? Can you see the billowy shapes around the fleur-de-lys points as stylized representations of puffs of wind?
Featured image: Portolan chart, Jorge de Aguiar (1492).
[1] See, for example, Alfred Hiatt, ‘From Hull to Cartage’: Maps, England and the Sea’, in Sebastian Sobecki ed., The Sea and Englishness in the Middle Ages (Brewer, 2011).
What has historical pregnancy testing got to do with arctic exploration and the expedition to rescue John Franklin, lost during his attempt to find a Northwest Passage? The idea of finding a Northwest passage, between the Pacific and the Atlantic oceans, was a long-held fixation; as early as the sixteenth century explorers had dreamed of it. Attempting to make that idea a mapped reality was perilous; those who attempted it were working at the extreme limits of endurance and at the edge of the known charted world. In contrast to the exotic problem that that search held out, the problem of pregnancy diagnosis was much more familiar, every day and domestic. Yet it was equally elusive.
Elisha Kent Kane. Wood engraving by [S. T.], 1856. Image from Wellcome Collection
These two exploratory fields are brought together in the extraordinary biography of Elisha Kent Kane, an adventurer, naval officer and doctor who was enlisted to go on Grinnell’s expeditions to find John Franklin in 1850 and 1853, the second of which he led. He graduated from the medical faculty of the University of Pennsylvania in 1842. The dissertation that he submitted as part of his training concerned experiments he conducted on the urine of pregnant and lactating women. His account of these experiments is full of odd case studies of women in the Philadelphia hospital, which give us an extraordinary glimpse of unpregnancy in the past.
In my Conceiving Histories project I am interested in the difficulty of diagnosing pregnancy and the time of not knowing – the am-I-aren’t-I time (that’s what I refer to as ‘unpregnancy’). I think that looking at the past before modern diagnostic technologies were available can give us ways of thinking about the times when our testing technologies aren’t useful, in the so-called two week wait before a pregnancy test, say, or in the weeks waiting for a viability scan. How did people try to know the body before our dipsticks and scans? At the very least I think that their endeavours testify to the fact that unpregnancy is a thing, that a state of indeterminacy is reasonably common, and that our abiding sense of a clear binary between not being pregnant and being pregnant is not exactly or not always how the (un)reproductive body is experienced.
One persistent idea, available throughout ancient, medieval and more modern medical writing, was that it might be possible to diagnose pregnancy by looking at and analysing urine in different ways. Of course urine testing has turned out to work like that, as it was always imagined it would. Technologies have to be imagined before they can be realised and so it has proved in this case.
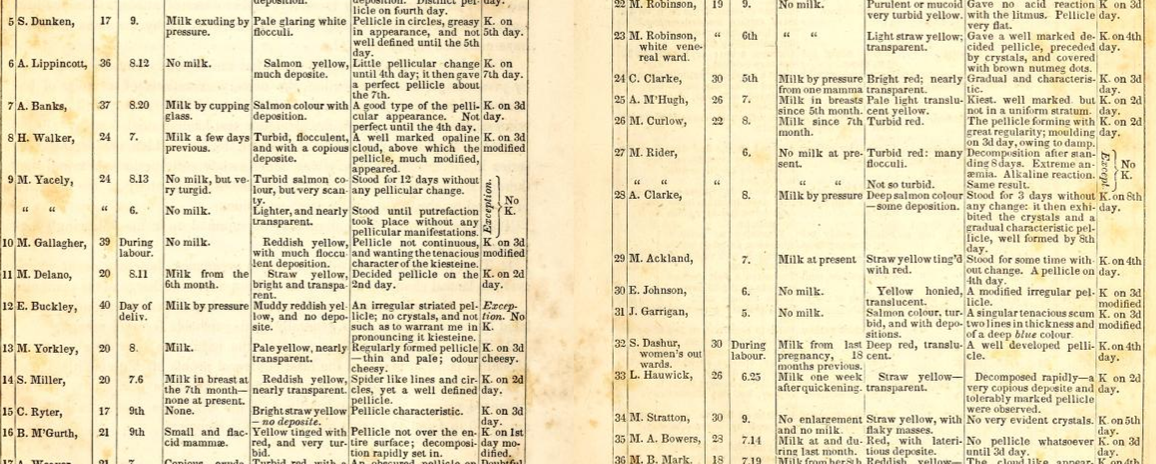
Kane was impressed by work that had been done by a French scientist Jacques Louis Nauche in 1831. Nauche had identified a substance in the urine of pregnant women which he named Kiesteine. This is a word made from the Greek word for conception, κύησις [kyesis], made to look technical by adding -ine, an inflection which was being used to name elements and other substances in a new chemical vocabulary (think of words like chlorine and bromine and so on). Kiesteine was a precipitate which appeared in pregnant urine which had been allowed to stand. It formed a pellicle, a skin or scum, on the surface of the urine. That sounds pretty disgusting but the way Kane describes it makes it sound rather beautiful:
…a continuous scum of an opaline white or creamy appearance, with a slight tinge of yellow, which gradually becomes deeper and more decided. The uniformity of this colour, however, is generally broken by granulated spots of a clearer white, giving it a dotted or roughened aspect. The crystals of the forming stage now appear like shining points, and I have sometimes found numerous small brownish specks, sprinkled over the surface, not unlike the gratings of nutmeg.
Kane did experiments on the urine not only of pregnant women but also lactating women in the hospital and also checked his findings by doing studies of other test groups: people with pathological conditions of different kinds. He found that kiesteine could be found in the urine of pregnant women and that in lactating women it could sometimes be found, especially during weaning or when breast feeding stopped for another reason. Kane recognised his work to be operating in a long tradition extending back into the medieval and classical past. He appreciated that something very like Kiesteine had been described by medical writers like for example Avicenna, writing in the early eleventh century, and carried into Western medical literature. Kane noted that writing on urine often described pregnant urine as containing clouds, like carded wool, soft and webby. Carding wool is not something many of us do now, but it would have been a very familiar description to people before the industrial revolution.
Kane’s tables of data, ‘Experiments on Kiesteine’.
The case studies are perhaps the strangest part of Kane’s thesis and give us an oblique view of women caught in the in-between of unpregnancy. Kane reproduces some of his data in tables (above) and some as narrative histories. Those narratives are all about how he used kiesteine correctly to diagnose pregnancy in hard cases. We are sometimes given the names and ages of these women, and sometimes not; we are often told in which ward they were being treated. In some cases we know that these women are black or white, because they are patients in segregated wards. Some of them have had many children and are already mothers. The list includes women who are deliberately pretending to be or not to be pregnant, and others who are mistaken about their own conditions; in some cases Kane is just sorting those that are from those that aren’t, with little comment about what the women themselves thought, believed or tried to pretend. His testing technique is clearly particularly useful for achieving negative results which are often more elusive. After all, the birth of a baby is the surest sign of pregnancy.
I find these case studies hard to read. The details of these women’s lives rip vividly across time, but of course we have no way of finding out about how they felt either about being pregnant or not or winding up as a test subject in Kane’s experiments. The first on Kane’s list, Helen Anderson, may be a sex worker; she is being treated on the hospital’s venereal ward for gonorrhea and Kane describes her sexual habits pejoratively as ‘promiscuous’. Kane successfully diagnoses her pregnancy and she gives birth to a baby prematurely. Isabella Smith is 25 and comes into Kane’s data set from the white obstetrical wards. She seems to have a well-advanced pregnancy but it hasn’t been possible to do an internal examination because she has ‘epileptic paroxyms’ which result in ‘her temporary removal to the women’s lunatic asylum’, where Kane acquires a urine sample. Kane records her test as a negative which satisfy him ‘that she was an imposter’. Then, ‘during a well simulated paroxysm of epilepsy, her dress gave way, and disclosed an abundant mass of hair padding ingeniously arranged over the abdomen’. There is no hint as to her motive, why she might need to pretend. Another test subject, Maria Hero, is just 15 and borrows urine samples from her neighbour who isn’t pregnant, to hide her condition from the doctors.
Little disguises the note of triumph that Kane sounds at being able to see through women’s deceptions or, in cases where there is no attempt to deceive but a genuine confusion, to read through misleading symptoms. Clearly he understands his success to be measured in the admiration of his male colleagues who are sending him samples and marvelling that he can invariably make a correct diagnosis. Of seven samples they ‘presented under fictitious names, and at a distance of two miles from the place where they were voided’, Kane could perform the trick of correctly picking out the four cases of pregnancy. He shows no empathy for the women he researches, or any concern about the emergencies which may have brought them into his case notes.
Of the nine narratives that Kane details, three are pregnant and clearly resistant to being so, like Maria Hero. The others are not. One is the ‘imposter’ with the hair padding I mentioned above, but there are an astonishing four cases (of just nine) who clearly believe themselves to be pregnant, in whom ‘the evidences of pregnancy were well marked’, but who aren’t. The longest of Kane’s case note entries concerns 37-year-old Mary Welsh. Not only do her periods stop – they are irregular anyway– her abdomen is swollen, milk has come into her breasts, and she feels foetal movements. She is multiply examined internally and externally; doctors including Kane have listened with a foetal stethoscope for a uterine ‘souffle’ or foetal ‘pulsation’. These different physical examinations prove inconclusive. Kane’s observations of her urine convince him that she is not pregnant despite all this ambiguity; ‘much against her own wishes and those of her fellow patients’ he discharges her to the female working wards. She is undelivered of this phantom pregnancy at the time Kane writes, perhaps as much as year after she began to suffer.
Elisha Kent Kane. Engraving by D. G. Thompson, 1858, after J. B. Wandesforde. Image from Wellcome Collection.
Many years later, when Kane kits himself out for his arctic adventure, he clearly still sees himself as an experimental scientist, and his task as not only about finding Franklin. As well as making himself a wolf-skin robe, which he says ‘wandered down’ to him from the ‘snowdrifts of Utah’, and getting some good warm knitwear, he buys himself ‘instruments for thermal and magnetic registration’. His journey notes are full of his findings and thoughts on all sorts of natural forms and phenomena, as well as the indigenous people that his party meets on its way. On his trip, he turns his considerable powers of observation and description from the specimen bottle to these exotic novelties. Kane notes, though, that there is much that surpasses his ability with words, so that he confesses himself
…amused with the embarrassments which my journal exhibits in the effort to describe [the icebergs]. Certain it is that no objects ever impressed me more. There is something about them so slumberous and so pure, so massive yet so evanescent, so majestic in their cheerless beauty without, after all, any of the salient points which give character to description, that they almost seemed to me the material for a dream, rather than things to be definitely painted in words.
Kane’s expedition never did find Franklin, just the remains of his winter camp. Experiments into kiesteine went nowhere. Here, then, are two dead ends in the map of history. Both eluded the efforts of Kane and others to define and settle them. Whatever clarity kiesteine gives Kane, it is firmly dismissed as nonsense by the scientists in the early twentieth century, who developed accurate animal tests. Neither his work, nor that of others who were also experimenting with kiesteine, fed into modern diagnostic practice. Experiments into kiesteine were overtaken by other means and ways of discovering pregnancy.
Kane’s account of the unpregnant women in Philadelphia Hospital show us of course that men had a curiosity and investment in clarifying and settling pregnancy diagnoses, but there are also hints here about how it also must have mattered to women, many of whom were suffering with symptoms but never delivering. For scientists like Kane, unpregnancy was an exciting exploration into uncharted and unknown places, full of puzzles and wonders, but for the women on whom he experiments, unpregnancy was a very cold and hostile wilderness in which some were hopelessly lost and from which there was little or no hope of rescue.
References:
Elisha Kent Kane, ‘Experiments on Kiesteine’, American Journal of the Medical Sciences 4 (1842): 13-38.
Elisha Kent Kane, The United States Grinnell Expedition in Search of Sir John Franklin: A Personal Narrative (Philadelphia: Childs & Peterson, 1856).
The figure of the child turning itself to the birth 2016, 21 x 29.7cm, photography
Our session featured Isabel talking about Mary Tudor and her two false pregnancies, and Anna introducing people to her work on Mary’s story. Anna also had some of these pieces in the Fertility Fest exhibition, one of which you can see here.
We were followed by the amazing Emma Cunniffe, who was talking about her experience of playing the role of Queen Anne, in a play of that name by playwright Helen Edmundson. She read from the play, talking particularly about the question of grief and how it affects the different characters very differently.
We were joined in discussion, after our presentations by Julia Bueno and Tracey Loughran. Julia is an experienced psychotherapist, who specializes in fertility issues. She is currently writing a much-needed book on miscarriage, using her experience of helping her clients in the aftermath. Tracey is an academic historian at the University of Essex. She has published a crucial collection of essays on the history of infertility and leads a Wellcome Trust funded project on women’s health in the twentieth century.
The audience was great, asking us really hard and interesting questions. Someone asked about what sort of oral histories were being collected now by historians. One person commented on how quickly women’s horizons of expectation in relation to family had changed between recent generations. Another noted how different ideas about infertility were in other cultures (her example was Spain as compared to the UK). One person asked about how far we could think about much older historical cultures as ‘closer to nature’. These have left me with much food for thought about how to move forward in our future research into un-pregnancy.
The Fertility Podcast also podcast other events and sessions at Fertility Fest, so you can catch up on lots of what went on at the festival, there.
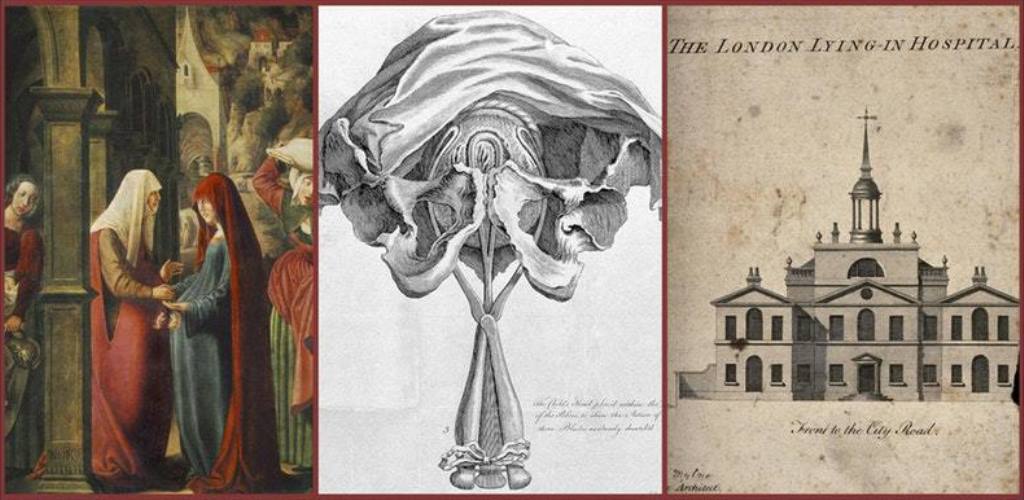
Imagine a dark Gothic building, with walls a hundred foot high. Inside are one hundred female experimental test subjects, ranging in age from fourteen to forty five. The staff over-seeing this curious institution are recruited from monasteries and relied on to keep accurate scientific data. No men are allowed into this hospital, part from male midwives of scrupulous integrity. Their visits are part of a clinical research trial, to discover the exact length of human gestation, and from when and what to date pregnancy.
This is the bizarre science-fictional building imagined by Robert Lyall, who was a nineteenth-century physician, botanist and traveller, in response to the confusing medical evidence presented in the Gardner peerage dispute heard in the House of Lords 1825-6.
This story testifies to how difficult it sometimes was for historical physicians, let alone lay people, to diagnose pregnancy reliably and early. The medical evidence gives us all sorts of information about how pregnancy was dated at the beginning of the nineteenth century, showing that there was little agreement between practitioners about the best way to do it. Just like today, people in the early nineteenth century understood themselves to be living through a hypermodern age, when all sorts of strides were being made in technology and science: for example, in steam power, electricity, and air flight. And yet, for all this progress, it still wasn’t possible to get a fix on the reproductive body, which was so familiar and close to hand. It felt anachronistic, Robert Lyall tells us in his eccentric commentary on the Gardner case.
We might reflect on a similar feeling of anachronism that people, and particularly women today encounter in the two week wait, in the time after embryo transfer or ovulation and before a pregnancy test is reliable. Just as women search their bodies for pregnancy signs and symptoms, Robert Lyall speculates on whether conception would feel like ‘the sting of a wasp, or like the bite of some other insects’. But, in the time before it’s possible to test, women today are in the same position as those in the past who didn’t have the test at all.
I have enjoyed finding out more from this network about historical midwifery, childbirth and pregnancy. My part has to be interject the thought about the risks of not giving birth, which are often not the focus of historical inquiry. Listening to others in this group considering the historical management of birth risk, has forced me to reflect on the more often psychological, social and perhaps insidious risks posed by un-pregnancy.
That project is now hosting a new exhibition which opens at the Thackray Museum, in Leeds on 15th June, and will eventually tour to London and Brighton. It’s great to see this on-going conversation coming to fruition.
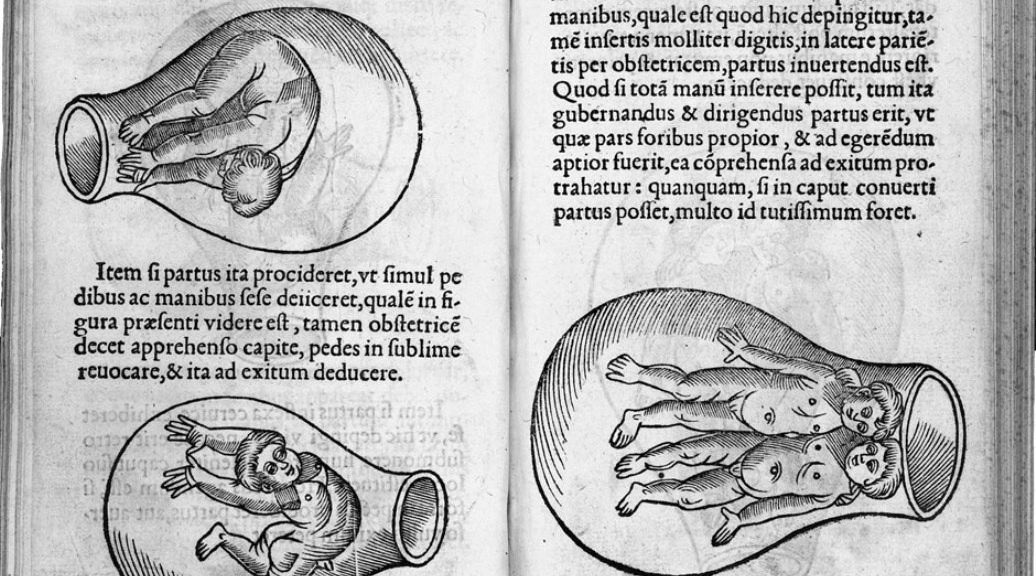
Featured image: Eucharius Rösslin, De partu hominis, et quae circa ipsum accidunt (1532).
A couple of weeks ago, Conceiving Histories took part in a ground breaking fertility education pilot, Making Modern Families, led by Fertility Fest and incorporating expertise from fertility scientists, arts-education professionals, artists, theatre practitioners, and young people. Fertility Fest is headed up by two visionary women at Fertility Fest, Jessica Hepburn and Gabby Vauntier-Farr, and their education initiative is funded by the Arts Council of England and the Wellcome Trust.
It was a huge privilege to be part of this extraordinary interdisciplinary group rethinking fertility education for today. We learned a huge amount during an energising week of discussion.
We met every day for a week at the National Theatre Studios in London, working together to make arts-led workshops which would foreground and confront questions around fertility, addressing perceived insufficiencies in sex education. Sex education currently is primarily focused on helping people to avoid both unwanted pregnancy and sexually-transmitted infection. These, of course, are crucial aims and there is no desire to see those health message diluted. However, at the same time, it is important that people have a better sense of what fertility is and how they can protect and preserve it. Letting people know, before it becomes an issue for them, that conceiving isn’t always quick or easy is also an important message so that, when it does become an issue for them, they don’t feel alone or unusual, and they know how to help themselves and/or where to seek help from others. Furthermore, the project sets out to tackle misconceptions about how medical science might be able to help. The media is keen to report on scientific breakthroughs in relation to reproductive science and, of course, science can do wonderful things. However, there is a lot that is still unknown and lots that it cannot do to help people to become parents.
How can Conceiving Histories help with these very contemporary fertility questions?
We think that having a historical perspective on this issue can do a number of things:
* History can help us today to find a vocabulary for delay, disappointment and the unknown, a lost vocabulary. We often think that we are very different from people in the past, who had less knowledge and fewer technological solutions. Sometimes we can forget that experiences like loss and waiting are still with us; they are modern experiences. If we don’t acknowledge that they are, people can feel left behind or at odds with modernity. People in the past thought a lot about the unknowability and frustrations of the reproductive body. We can learn a lot from them.
* History can help us find a space beyond the self to reflect on our own desires and experience. The world is full of the stories of contemporary people and their struggles. These stories are important and useful to help us understand our selves. History, however, offers a separate and novel reflective space. In that space we can mobilise our intellectual curiosity, as well as our feelings about the human reproductive body, its place in culture, and in relation to our sense of self.
*History can help us reflect on science and medicine. What is it? What do we hope it can do for us? Does it want the same things for us as we want for ourselves? How did particular scientific emphases, understandings or technologies come into being? Can we get an objective or scientific fix on our reproductive bodies?
We used our workshop to explore the strange case of Mary Tudor, who was Queen of England from 1553 until 1558, and her two false pregnancies. We asked participants to think about Mary’s fantasies of pregnancy and how those fantasies were collective, driven as much by the people around her as by Mary’s own desire to be a mother and to secure her political lineage. Students spent their workshop time making images of Mary to reflect on the pressures on women to become mothers. Some students drew connections with modern monarchy and the emphasis on pregnancy in the coverage of royal marriages; others wanted to think about the messages that ordinary women today are given about becoming mothers, and perhaps particularly when they should become mothers. Mary’s story is extraordinary because it highlights the very powerful connection between the mind and body. Although our routine use of diagnostic technologies in the West has meant that cases like Mary’s are less common than they were, the close link between mind and body still exists, and looking after ourselves depends on our appreciation of that connectivity.
We are looking forward to seeing how this project develops and to participate in any way we can. We will continue to think about how the past can inform our reproductive present and futures. We are hugely grateful to have encountered the wonderful expertise (in science, theatre, arts, in education, and in making things happen) of all the other contributors in this important and valuable initiative.
We are really excited to be taking part in Fertility Fest later this year at the Bush Theatre, in London. Fertility Fest is an innovative arts festival, facing the difficult topics of fertility and infertility. There are 150 artists and fertility experts taking part, with a whole range of different events across six days in May (8th-13th).
The festival aims to:
Improve the understanding of the emotional journey of people who struggle to conceive
Improve the level of public discourse about reproductive science
Improve fertility education
Conceiving Histories is about understanding how history can contribute to contemporary fertility health. Modern technologies can, of course, help people to become parents; science can do amazing things. There are many things, however, with which it cannot help. In particular it cannot help us to wait, or to cope with disappointment. History and art, disciplines brought together in the Conceiving Histories project, offer an interesting space, beyond the self, from which to think about – and perhaps even to learn to tolerate – reproductive delay, disappointment and uncertainty.
Some of Anna Burel’s Conceiving Histories work will be featured in the fertility fest exhibition, which is on display across the festival’s six days. The work we’ve chosen to show explores a strange idea from the early nineteenth century for an ‘Experimental Conception Hospital’, an institution in which women would be experimented on in order to understand some of the mysteries of conception.
We are also excited to be taking part in a special discussion session on ‘Unpregnancy: Infertility before IVF’ with writer, psychotherapist and expert on pregnancy loss, Julia Bueno; actor Emma Cuniffe, who played Queen Anne in the acclaimed RSC production of the same name; and historian Tracey Loughran, who has co-edited a path-breaking book on the history of infertility, at Sunday 13th May, 11.45. We are interested to get their takes on history and how it can be used to think about contemporary fertility.
We will be talking about the work we have on display in the exhibition, and a bit more about the Experimental Conception Hospital story. We will be particularly focussing on how this odd institution might give us ways to think about the two week wait and the difficulties of diagnosing early pregnancy, and about science and the desire to get an objective fix on the body.
Anna and I went along to the Fertility Fest launch last Tuesday and there was a palpable buzz in the room. People are clearly as excited as we are to be joining the show. We were given a sneak preview of Camilla Whitehill’s inclusive and charming short play Aloe Aloe, directed by Lucy Jane Atkinson and performed by twelve actors, exploring modern families and the multitudinous ways they are made today. Then Jessica Hepburn and Gabby Vautier gave us their vision of the festival. They hope to change the world, they said; it was a moving call to arms.
Fertility Fest is about getting fertility and infertility talked about more, and talked about better. That’s got to be a good thing. I’m sure there will be sadness as well as positivity at the festival. Our own contribution will, I hope, entertain, but it is also dark and curious, disturbing, confronting the difficulties of the unknown and fantasies of science. Yet the launch was quite definitely an upbeat event. The room was filled with pastel balloons; we each held one as we had our photos taken, like party guests. Coincidentally, Anna and I have thought a lot about the shape of the balloon and its similarity to the uterus (perhaps we’ll tell you about that at the festival). We couldn’t help but see the balloons as so many coloured floating uteri, cheerfully bobbing up to the ceiling.
We welcomed 1372 visitors through the doors of the Conceiving Histories exhibition in November and December 2017. Amongst the many generous comments in the Peltz Gallery visitors’ book, people described the exhibition as: ‘compassionate’, ‘moving’, incredible’, ‘fascinating’, ‘evocative’, ‘heart-breaking’, ‘haunting’ and ‘emotional’.
Anna and Isabel took around six tour groups, hosted a gallery launch and an academic/artist symposium, The Pregnant Archive, with Dr Emma Cheatle of Newcastle. We took part in the Being Human Festival, the UKs first national festival for humanities research.
Cover image of catalogue
We are sending out copies of our exhibition catalogue to those who couldn’t make it but would have liked to. If you would like a free copy contact Isabel (i.davis@bbk.ac.uk) with your name and address and she’ll send one to you.
Isabel spoke to the amazing Natalie Silverman at the Fertility Podcast about the project in the lead up to our exhibition.
Four visitors were inspired to write blog posts about the exhibition:
Although our exhibition has closed, this isn’t the end of the project. Watch this space and follow us on Twitter to keep up with the project.
With special thanks to our funders: the Peltz Gallery, Birkbeck’s Centre for Medical Humanities and those philanthropic individuals who donated through our Kickstarter campaign.
With thanks to the Wellcome Trust and Birkbeck College who funded the research behind this exhibition.
With thanks too to all those who came, blogged, tweeted, gave us their feedback, told their friends and generally and in every way supported us.
THE PREGNANT ARCHIVE: Materialising Conception to Birth 30 November–1 December 2017
Two-day symposium and collaborative workshop, Birkbeck, University of London
Organised by Dr Emma Cheatle (Newcastle University) and Dr Isabel Davis (Birkbeck, UoL)
Funded by Newcastle University and Wellcome/Birkbeck ISSF.
DAY 1: THURSDAY 30 NOVEMBER 2017
11:00 Coffee
Introduction to exhibition, Conceiving Histories, by the artist Anna Burel
11:30 Introduction to the PREGNANT ARCHIVE by Isabel Davis and Emma Cheatle
11:45 Session 1: QUESTIONS OF CONCEPTION [Chair Isabel Davis]
20 minute papers from Shrikant Botre, Sara Read, Jesse Olszynko-Gryn
12:45 Questions and discussion
15:15 Tea
16:00 Session 3: BIRTH SPACES [Chair Emma Cheatle]
20 minute papers from Hermione Wiltshire, Sarah Fox, Edwina Attlee, Cathy McClive
17: 20 Questions and discussion
17: 50 Organisers’ Remarks
18:00 Drinks in the Peltz Gallery followed by dinner
DAY 2: FRIDAY 1 DECEMBER 2017
10:00 Coffee
10:15 Session 4: MATERIALS OF PREGNANCY [Chair]
20 minute papers from Rebecca Whiteley, Rosemary Betterton
10:50 Questions and discussion
[short break]
11:15 20 minute papers from Anne Carruthers, Karen Harvey, Magdalena Ohaja,
12.15 Questions and discussion
12:40 Session 5: ARTIST RESPONSES workshop / collaborative conversation
10 mins/person: Lana Locke, Leah Lovett, Jessa Fairbrother
13:30 Lunch and further discussions on future collaborations
14:45 Regathering and closing remarks with artists and speakers. Possible futures.
15:00 End
Recently I spoke to Natalie Silverman for The Fertility Podcast. Natalie has built up a great library of podcasts from all sorts of different contributors talking about fertility and infertility, from clinical practitioners to people with their own personal fertility stories. She is always looking for people to talk to. So, if you have a story to tell, perhaps you should get in touch with her. Why not follow the Fertility Podcast on twitter: @fertilitypoddy to get alerts?