A new global “soft power” ranking recently reported that the democratic states of North America and Western Europe were the most successful at achieving their diplomatic objectives “through attraction and persuasion”.
Countries such as the US, the UK, Germany and Canada, the report claimed, are able to promote their influence through language, education, culture and the media, rather than having to rely on traditional forms of military or diplomatic “hard power”.
Although the term “soft power” was popularised by the political scientist Joseph Nye in the 1980s, the practice of states attempting to exert influence through their values and culture goes back much further. Despite what the current soft power list would suggest, it has never been solely the preserve of liberal or democratic states. The Soviet Union, for example, went to great efforts to promote its image to intellectuals and elites abroad through organisations such as VOKS (All-Union Society for Cultural Relations with Foreign Countries).
Perhaps more surprisingly, right-wing authoritarian and fascist states also used soft power strategies to spread their power and influence abroad during the first half of the 20th century. Alongside their aggressive and expansionist foreign policies, Hitler’s Germany, Mussolini’s Italy and other authoritarian states used the arts, science, and culture to further their diplomatic goals.
‘New Europe’
Prior to World War II, these efforts were primarily focused on strengthening ties between the fascist powers. The 1930s, for example, witnessed intensive cultural exchanges between fascist Italy and Nazi Germany. Although these efforts were shaped by the ideology of their respective regimes, they also built on pre-fascist traditions of cultural diplomacy. In the aftermath of World War I, Weimar Germany had become adept at promoting its influence through cultural exchanges in order to counter its diplomatic isolation. After 1933, the Nazi regime was able to shape Weimar-era cultural organisations and relationships to its own purpose.
Leni Riefenstahl, Hitler’s film-maker. Bundesarchiv Bild, CC BY
This authoritarian cultural diplomacy reached its peak during World War II, when Nazi Germany attempted to apply a veneer of legitimacy to its military conquests by promoting the idea of a “New Europe” or “New European Order”. Although Hitler was personally sceptical about such efforts, Joseph Goebbels and others within the Nazi regime saw the “New Europe” as a way to gain support. Nazi propaganda promoted the idea of “European civilization” united against the threat of “Asiatic bolshevism” posed by the Soviet Union and its allies.
As seen in Poland: a BNazi anti-Bolshvik poster.
Given the lack of genuine political cooperation within Nazi-occupied Europe, these efforts relied heavily on cultural exchange. The period from the Axis invasion of the Soviet Union in June 1941 until the latter stages of 1943 witnessed an explosion of “European” and “international” events organised under Nazi auspices. They brought together right-wing elites from across the continent – from women’s groups, social policy experts and scientists to singers, dancers and fashion designers.
All of these initiatives, however, faced a common set of problems. Chief among them was the challenge of formulating a model of international cultural collaboration which was distinct from the kind of pre-war liberal internationalism which the fascist states had so violently rejected. The Nazi-dominated European Writers’ Union, for example, attempted to promote a vision of “völkisch” European literature rooted in national, agrarian cultures which it contrasted to the modernist cosmopolitanism of its Parisian-led liberal predecessors. But as a result, complained one Italian participant, the union’s events became “a little world of the literary village, of country poets and provincial writers, a fair for the benefit of obscure men, or a festival of the ‘unknown writer’”.
Deutschland über alles
Despite the language of European cooperation and solidarity which surrounded these organisations, they were ultimately based on Nazi military supremacy. The Nazis’ hierarchical view of European races and cultures prompted resentment even among their closest foreign allies.
Jesse Owens after disproving Nazi race theory at the Berlin Olympics, 1936. Bundesarchiv, Bild, CC BY-SA
These tensions, combined with the practical constraints on wartime travel and the rapid deterioration of Axis military fortunes from 1943 onwards, meant that most of these new organisations were both ineffective and short-lived. But for a brief period they succeeded in bringing together a surprisingly wide range of individuals committed to the idea of a new, authoritarian era of European unity.
Echoes of the cultural “New Europe” lived on after 1945. The Franco regime, for example, relied on cultural diplomacy to overcome the international isolation it faced. The Women’s section of the Spanish fascist party, the Falange, organised “choir and dance” groups which toured the world during the 1940s and 1950s, travelling from Wales to West Africa to promote an unthreatening image of Franco’s Spain through regional folk dances and songs.
But the far-right’s golden age of authoritarian soft power ended with the defeat of the Axis powers. The appeal of fascist culture was fundamentally undermined by post-war revelations about Nazi genocide, death camps and war crimes. At the other end of the political spectrum, continued Soviet efforts to attract support from abroad were hampered by the invasion of Hungary in 1956 and the crushing of the Prague Spring in 1968.
This does not mean that authoritarian soft power has been consigned to history. Both Russia and China made the top 30 of the most recent global ranking, with Russia in particular leading the way in promoting its agenda abroad through both mainstream and social media.
The new wave of populist movements sweeping Europe and the United States often also put the promotion of national cultures at the core of their programmes. France’s Front National, for example, advocates the increased promotion of the French language abroad on the grounds that “language and power go hand-in-hand”. We may well see the emergence of authoritarian soft power re-imagined in the 21st century.
Conference Report – Crossing Borders: The Spanish Civil War and Transnational Mobilisation, Birkbeck, 30 June-1 July 2016
Earlier this summer, Birkbeck played host to a two-day conference on the international history of the Spanish Civil War. Crossing Borders: The Spanish Civil War and Transnational Mobilisation was funded by The Reluctant Internationalists research group, Birkbeck, Queen Mary, the University of Kent and the Royal Historical Society, and was organised in collaboration with the Cañada Blanch Centre for Contemporary Spanish Studies at the LSE. Bringing together over thirty scholars from the UK, Europe, the US and further afield, it set out to explore the origins and experiences of transnational mobilisation during the conflict and the immediate post-war period.
The first day began with a panel on the wide range of transnational actors involved in the war, from the Republican politicians who helped to establish the Popular Front movement whilst in exile in Paris in 1934 and 1935, to the international peace activists whose campaigns against aerial warfare encompassed both the Spanish and Chinese civil wars. Complicating the traditional focus on transnational mobilisation in favour of the Republican cause, the panel also discussed the involvement of fascist-dominated veterans’ networks in debates about international intervention, and the international left-wing mobilisation in favour of POUM activists imprisoned by the Republican regime.
The remainder of the day focused on the humanitarian and medical dimensions of transnational mobilisation during the Civil War. A number of papers focused on the thousands of Spanish refugees who were evacuated from Republican zones during the conflict, or who fled to France in 1939. Wartime evacuations were organised both by the Republican government and its allies, and by international humanitarian groups, but were hampered by the political tensions surrounding the conflict. The huge numbers of refugees stranded in France at the end of the war were housed in overcrowded and insanitary camps, with care provided by exiled Spanish medical professionals and by humanitarian organisations. For the international humanitarian community, the Spanish Civil War represented both an intense political, financial and logistical challenge, and a crucial step in the development of new models of humanitarian activity. The conflict itself left thousands of people exiled, bereaved or permanently disabled, with its legacies living on both inside and outside Spain through such individuals well beyond 1939.
The second day shifted focus towards the military dimension of transnational mobilisation. The first panel on propaganda highlighted the ways in which the thousands of Moroccan troops who fought with rebel forces were portrayed and instrumentalised in propaganda on both the Republican and rebel sides. It also demonstrated how the Spanish Civil War came to play a central role in the anti-Bolshevik cultural activities of Nazi Germany. This was followed by two panels which focused on the experiences of the transnational military volunteers who took part in the conflict. The first focussed on the International Brigades, providing a new perspective on this oft-studied topic by highlighting the relations between volunteers of different nationalities within individual battalions, and on the experiences of international volunteers after their return home. It also featured a fascinating presentation on SIDBRINT, a new digital archive on the International Brigades hosted by the University of Barcelona which provides an invaluable resource for scholars interested in the transnational history of the Spanish Civil War. The second panel took a global perspective on transnational military mobilisation, examining the experiences of Arab and Jewish volunteers who fought with Republican forces, and the experience and memory of a Basque town which played host to both German and Italian troops during the conflict.
The final panel of the conference focused in on the transnational lives and experiences of individuals involved in the Spanish Civil War. Artists such as the Hungarian photographer Kati Horna drew on their experiences of the war to explore the importance of internal and external borders for those who had lived through it. The lives of other individuals and groups continued to be affected by the Spanish Civil War long after formal hostilities had ended, including the Spanish and Catalan women imprisoned by the Nazis at Ravensbrück during the Second World War, and the Czech and Slovak communist volunteers whose post-war political and emotional lives were shaped by their experiences in Spain.
The theme of transnational lives also lay at the heart of the conference’s keynote delivered by Helen Graham (Royal Holloway). A well-attended public lecture hosted by the Institute of Historical Research and introduced by Paul Preston (LSE), this fascinating lecture used the lives of five individuals to explore the significance of the Spanish Republic cause to the continental wars of social change which took place between 1936 and 1948. A podcast of the lecture is available online, and you can find abstracts for all of the conference papers and information about individual speakers here.
Dora Vargha and David Bryan have written an article on the recent appearance of diphteria in Spain. The re-emergence of this infectious disease, which had not been recorded in the country in the last 28 years, has instigated heated debates regarding the impact and legitimacy of the anti-vaccination movement, and Vargha and Bryan have addressed this topical issue in the context of the general history of vaccination as well as of Spain’s troubled legacy of authoritarianism and public health. The article has been published in English on the UK website The Conversation, and in Spanish in El País.
‘Strangling angel’ of diptheria caught Spain off guard – here’s how
The return of diphtheria in Spain after nearly three decades highlights the challenges posed by infectious diseases that had been mostly eliminated from Europe.
Falling vaccination rates, complex population movements, and the disappearance of international health practices perceived as redundant, all contribute to the emergence and spread of infectious diseases that were thought forgotten. At the same time, such public health crises throw light on the delicate relationship between state and citizens, and competing concepts of responsibility for health.
A six-year-old boy from the Catalan town of Olot was admitted to hospital suffering from diphtheria last week. This was the first case of the disease recorded in Spain for 28 years. The boy, who is in a critical but stable condition in a Barcelona hospital, had not been vaccinated due to his parents’ concerns about the safety of the vaccine. They now say they feel tricked by the anti-vaccination groups which had originally stoked their fears.
Diphtheria, now a rare disease in Europe, is a serious, potentially fatal disease caused by bacteria that can cause heart failure, pneumonia and paralysis of the muscles used for swallowing. Up until the 1920s it was one of the leading cause for death in children, sometimes referred to as “strangling angel”, because the bacteria can create a pseudo-membrane in the airways, causing death by choking.
It was widespread in Spain during the first half of the 20th century, particularly following the physical and economic devastation caused by the Spanish Civil War. Over 27,000 cases of diphtheria were recorded in 1940 alone. Improving infant health was officially a priority for the new Franco regime, and cases did reduce significantly in the post-war era. However, Spain’s impoverished and fragmented public health system failed to make the rapid progress towards eradication achieved by its western European neighbours, with almost 250 new cases a year still reported in the late 1960s. A comprehensive vaccination programme was finally implemented in 1966 and until last week, there had been no diphtheria cases recorded since 1987
Russia to the rescue
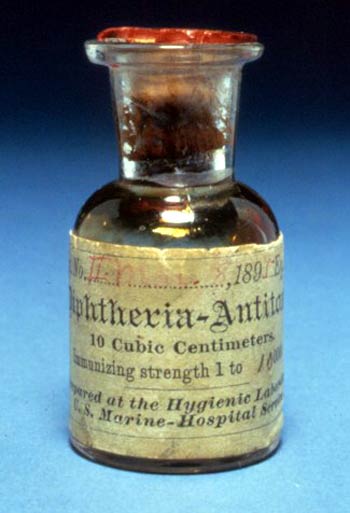
As diphtheria had been eliminated in Spain for the last three decades, stocks of the anti-toxin needed to treat the disease are no longer available in the country. This anti-toxin, listed as an “essential medicine” by the World Health Organisation, is increasingly unavailable due to the disease’s rarity and because, as a blood-derived product, its production is highly regulated.
Diphtheria Antitoxin from 1895 “Antitoxin diphtheria” by Unknown – A Short History of the National Institutes of Health. Licensed under Public Domain via Wikimedia Commons
For instance, in the US there are no licensed anti-toxin products available in the whole country, and in case of diphtheria an unlicensed Brazilian product is used by the CDC under investigational new drug status, which basically provides an exemption from federal regulation. In Europe, some public health experts have called for the establishment of a central EU stockpile that all countries can access in times of emergency.
This time, Spanish health authorities were forced to look abroad for supplies, which were personally flown in from Moscow by the Russian ambassador to Madrid. The difficulties in locating and supplying the relevant anti-toxins highlight how quickly international structures can break down once a disease has been eliminated in a particular country and has disappeared from the authorities’ radar.
The recourse to diplomatic channels and the ad hoc supply of medication echoes the chaotic situation more usually associated with times of war and international emergency. A look into the Spanish government archives reveals that during the World War II, for example, Spain’s small West-African colony in what is now Equatorial Guinea faced a dangerous outbreak of Yellow Fever. Facing the collapse of its economy and wartime disruption to international supply, the Spanish government struggled to secure basic medication and to distribute the relevant vaccines both at home and in its overseas colonies.
Help eventually arrived from the local British Consul who agreed to fly to Lagos and bring back supplies of the vaccine in thermos flasks. While these kind of ad hoc solutions may have been a necessary during a time of international conflict, they seem profoundly out of place in today’s apparently more orderly international system.
A lingering presence
It was no coincidence that the anti-toxins were available in Russia. Diphtheria cases had begun to fall in the Soviet Union following the introduction of universal childhood immunisation in 1958. By the mid-1970s they had plummeted to an all-time low, approximately the same level as the US. However, changing immunisation schedules contributed to a rise in diphtheria in the 1980s, partly because of reduced levels of public support stoked by a strong anti-vaccination movement that channelled distrust in the state during the period of perestroika. With the collapse of the Soviet Union and much of its public health services, especially in the newly independent states, a severe epidemic broke out in 1993.
Shortages in vaccine supply, economic hardship and mass population movements all contributed to the outbreak and the difficulties authorities faced in controlling it. Eventually diphtheria in Russia and the former Soviet states was brought under control through international cooperation between governments, NGOs and UN agencies. Since then, the former Soviet republics and Russia have remained the only area of Europe where diphtheria is still a public health concern. Although no longer in epidemic proportions, the lingering presence of the disease led Russian authorities to keep stocks of diphtheria anti-toxin readily available.
Spain’s fascist past complicates the debate
Long-forgotten diseases that make a comeback also bring to light problematic relationships between citizens and the state. Recent American anti-vaccination movements highlight conflicting ideas of individual and public health, while Spain’s authoritarian legacy has coloured the vaccination debate in the country. This week Luis Garciano, economic spokesman for Spain’s new centrist party Ciudadanos (Citizens), said that unvaccinated children should be withdrawn from school and their parents fined and stripped of benefits.
Garciano’s comments have been denounced as “neofascist”, and anti-vaccination campaigners have frequently drawn parallels between the idea of obligatory vaccination and Spain’s fascist past. For them, the right to reject vaccination is a freedom that should be protected in the era of democracy.
The return of diphtheria to Spain mirrors the measles, TB and other infectious diseases in Europe and the US. When diseases disappear due to high vaccination coverage, the national and international public health infrastructures needed to deal with them often also whither away.
When distrust in public health organisations and practices or the break-down of relationship between state and citizens give way to faltering vaccination rates (whether through anti-vaccination movements or through lack of access to vaccines), forgotten diseases can make a quick comeback. The case of diphtheria reminds us of the very real stakes at hand when infectious diseases re-emerge and throw light on the personal, national and international consequences of declaring the end of a disease.
On March 12 and 13, the University of Lausanne hosted a thought-provoking and intellectually rich conference on the ‘Globalization of medicine and public health: economic and social perspectives (1850-2000).’ Convened by Sanjoy Bhattacharya (University of York, UK), Thomas David (University of Lausanne, Switzerland), Pierre-Yves Donzé (Kyoto University, Japan), Davide Rodogno (Graduate Institute of International and Development Studies, Geneva, Switzerland), this inter-disciplinary meeting aimed to explore the roots, development and consequences of the intensive globalizing trends in medicine and public health since the mid-nineteenth century. As Davide Rodogno and David Thomas said in their opening remarks, the conference sought to provide a critical analysis of the emerging historiography of global health and narratives of globalization, primarily by connecting the history of public health with other approaches such as business and economic history, history of medicine, international history etc. Moreover, the conference aimed to move away from linear and simplistic narratives of international cooperation and harmony, and to study international health organizations as spaces of interrogation, contestation, opposition and imposition of ideas.
The first panel addressed a score of these themes and opened up a number of key questions in the historiography of global public health. Anne-Emanuelle Birn (University of Toronto, Canada) discussed complex ties between philanthropic organizations and global health agencies through the prism of the fraught relationship between two of the most important actors in this field – the Rockefeller Foundation and the WHO. In her analysis of the ups and downs in their cooperation between the 1940s and 1980s, Birn examined the RF’s (often indirect) role in defining the WHO’s approaches and priorities, its participation in the WHO’s personnel, and emphasized the key moments as well as tensions, conflicts and dilemmas in the relations between the two institutions. Her paper explored how these developments affected global health initiatives in the second half of the twentieth century, and how they shaped the current role of philanthropy in the field of global health. Erez Manela (Harvard University, USA) discussed the WHO’s campaign for the global eradication of smallpox in the 1960s and 1970s. Focusing primarily on the US perspective, Manela examined the circumstances of this signal event in the history of global health in the second half of the twentieth century, and asked how this programme managed to achieve its goal of eradication on a global scale in the midst of international conflict, when so many similar initiatives had failed. Manela placed the smallpox eradication programme in the context of the US-Soviet Cold War rivalry and the growing role of the global South in international politics following the de-colonization. A transnational network of experts succeeded in co-opting governmental power and the backing of inter-governmental agencies for the project of small pox eradication at the very moment when the US sought to improve its vulnerable international status, while the programme of international development gained increasing importance for the US government as a tool for containing the spread of Communism in the newly independent countries in Asia and Africa. Nitsan Chorev (Brown University, USA) presented her research on the emergence in the 1970s and 1980s of remarkable local pharmaceutical sectors in East Africa, and explored the structure and development of local pharmaceutical production in Kenya, Uganda and Tanzania in a comparative perspective. According to Chorev, the development of local pharmaceutical manufacturing was seen as an important industrial goal in these countries, as they hoped to free themselves from their dependence on multinational companies and to secure access to necessary medicines. Chorev emphasized three interrelated factors that contributed to significantly different levels of success of local pharmaceutical industries in the three countries: state policies, transnational ties and foreign aid in support of state policies, and capable local entrepreneurs with cross-national ties (the key role was here played by ethnic minorities, for instance Indian Kenyans with their educational ties to the UK and India and work experience multinational pharmaceutical companies). The discussion following the panel was rich and vigorous, and it explored the difference and similarities between the concepts of global and international, but also emphasized the missing link in all three presentations – the Soviet perspective.
The second panel sought to focus on “non-Western visions” in the history of global health. Marcos Cueto (Casa Oswaldo Cruz, Brazil) shed light on the establishment and role of the WHO’s African Regional Office (AFRO) in the 1950s and 1960s, and placed the history of this important regional health agency in the context of the Cold War rivalries and the ongoing struggle for independence in sub-Saharan Africa. While initially this office was led by European experts in tropical medicine, its activities and personnel soon reflected the changing political and social realities in Africa, and this led to the increasing number of African personnel and African member-states. AFRO produced important studies on malaria, yellow fever and onchocercasis, and contributed to the revival of tropical medicine as a discipline, but Cueto’s presentation offered a critical analysis of the complex political role and achievements of this regional agency. On the one hand, the existence and activities of AFRO may have indirectly helped the independence processes in the 1960s, but it also re-produced the dependency of the south of Africa on Western, colonial models, and encouraged problematic discourses in which the newly independent countries of sub-Saharan Africa were constructed as the most underdeveloped and anarchic region in the world in need of a new form of humanitarianism, while AFRO was constituted as an island of (Western-style) modernity and progress. Monica Saavedra (University of York, UK) presented her research on the involvement of Portuguese India in the WHO’s South-East Asia Regional Office, in the final years of the Portuguese colonial rule. Saavedra showed that the WHO and SEARO were not merely forums for scientific and technical exchange and cooperation in the area of health, but also an international political stage where Portugal struggled to lay claim to Portuguese India and to legitimate its rule. This ambiguous relationship with SEARO resulted in political interests overshadowing the health needs of the population, so that official sources were dominated by political manouvres and agendas. The SEARO archive reveals a selective way of dealing with the international health affairs, and illustrates Porugal’s efforts to keep a flimsy balance between international approval and self-interest.
The third panel dealt in some detail with the history of pharmaceutical practices, initiatives and marketing in a global perspective. Jeremy Greene (Johns Hopkins University, USA) presented his research on critical discourses regarding the uneven distribution of access to life-saving pharmaceuticals in different parts of the world between the 1960s and 1980s. Greene explored the key discussions of the role that access to medicines played in international political and health development, and looked at positions of a number of stakeholders – doctors, policymakers, lawyers, manufacturers – in this global mapping of therapeutic inequalities. Julia Salle Younge (Hosei University, Japan) traced the emergence of a global vaccine industry model. According to Yongue, combination vaccines have become the global standard of vaccination in all developed nations — save one. Her presentation then traced the process that led to the formation of a global model for the vaccine industry while comparing two distinctively different cases, the French vaccine industry, which played a central role in the acceptance and propagation of combination vaccines and the Japanese vaccine industry, whose government, until only recently, has promoted the ‘de-combining’ of vaccines as the best means of preventing adverse reactions. The final speaker of the panel, Johanna Conterio Geisler (Birkbeck, UK), provided the sorely missing Soviet perspective and countered the historiographical narratives of the Soviet Union as increasingly isolated and isolationist in the interwar years. Her research explored the development of Soviet pharmaceutical industry in the global context of the 1920s and 1930s, and looked at how Soviet medical and health experts engaged with Western networks and approaches. They actively sought external influences and Western – US – models in order to spur the development of pharmaceutically crucial agricultural products and raw materials in the Soviet peripheries, and aimed to prevent the Soviet dependence on international pharmaceutical monopolies. While Soviet borders were closing down, outside influences continued flowing in.
In the fourth panel, focusing on actors and networks, David Thomas and Davide Rodogno discussed their ongoing project on the history and genealogy of public health fellowships in the twentieth century. They sought to connect the post-WW2 WHO international fellowships programme to its predecessors – the Rockefeller Foundation and UNRRA fellowships. Their research explored continuities and ruptures in this history, and focused on the concepts of human capital and development which informed and shaped the structure and goals of the different health fellowship programmes across the twentieth century. Clifford Rosenberg (CUNY, USA) analyzed the RF International Health Board’s attempt to establish a field programme in French Algeria in the 1920s, following the successful anti-TB programme it funded and ran in France during WWI. Rosenberg’s research explored this failed attempt in a political and colonial perspective, and placed the RF’s initiative in the context of the emerging international institutions and French and Algerian colonial patronage networks. Paul Weindling (Oxford Brookes, UK) presented his research on the RF’s social medicine healthcare experiments in the twentieth century. His paper focused on the RF-funded schemes in Natal, South Africa, in the 1950s. Weindling traced the RF’s efforts to establish a Department of family practice at Durban, the University of Natal, in a new medical faculty for non-white students, and its attempts to obtain guarantees that the non-white graduates would get government posts. While the Durban scheme ultimately failed in the context of the South African apartheid, Weindling argued for its great significance for understanding the history of the RF’s involvement in social medicine healthcare experiments, and he related the Natal health centre to other earlier attempts of the RF to combine primary healthcare with rural development and cultural and social factors.
The subsequent panel dealt with a variety of historical approaches to analyzing ‘Diffusions and models’ in global healthcare. Thomas Zimmer’s paper addressed the history of the Malaria Eradication Programme in the 1950s and 1960s, and specifically explored the role of the World Health Organization in the development and implementation of this initiative. Zimmer (Freiburg University, Germany) argued that, although the WHO financial and material contributions to the MEP were significantly lower than those of the main donor countries (such as the US), the WHO played a fundamental role in coordinating and codifying the Programme by establishing pilot projects which served as future models, lent legitimacy to the very idea of eradication, served as an intermediary between donor and developing countries, and was pivotal in evaluating ongoing projects. The paper concluded that the global malaria eradication was ultimately a WHO project, although the WHO could not have possibly launched or run it by itself and was at mercy of the ebbs and flows of international politics. Pierre-Yves Donze discussed the theme of diffusion and globalization of health models from a slightly different perspective – that of economic entrepreneurs and the history of industrial business. At the centre of Donze’s story was the German electro-medical equipment maker Siemens-Reiniger-Werke and its attempts to re-enter non-European (Latin American, as well as Asian and African markets) in the aftermath of WWII through the project of hospital construction. Instead of merely exporting goods, SRW organized and directed an informal association called Deutsche Hospitalia, which gathered around thirty German manufacturers. They were all involved in constructing and fully equipping the final product – the German hospital, which was then offered to the local governments. Donze analysed the initiative in the context of globalizing trends in medicine, and discussed how SRW contributed to these trends. Yi-Tang Lin (University of Lausanne, Switzerland) critically analysed the nature and production of WHO health statistics in different regions and areas, questioning the value of statistics as neutral markers of local health programmes and placing them in proper socio-political contexts. Lin concluded that the WHO’s strategy of standardization was not making a unique standard, but giving different instructions to countries with different public health administration capacities, and using statistics as a tool for legitimizing health programmes in different countries. Moreover, the WHO forged a network of knowledge transfer by providing fellowships for national health statisticians, inaugurating short-term training centres, and employing a statistician or economist for every regional office.
The final panel of the conference was titled ‘The world as a laboratory.’ Agata Ignaciuk (University of Granada, Spain) presented a comparative study of the leading European and US pharmaceutical companies’ strategies and practices for marketing the contraceptive pill in Francoist Spain and socialist Poland in the 1960s and 1970s. Although the two markets were radically different from the West European and American ones, as well as form each other, Ignaciuk was able to identify striking similarities. In the Spanish case, although sale and advertising of contraception had been banned until 1978 and the pill was marketed as a therapeutic drug, the pharmaceutical strategy was not fundamentally different from that practiced in Western Europe or the US, and focused on normalizing the idea of family planning among physicians and the broader public. According to Ignaciuk, this helped legitimize the idea of contraception in Spain, and aided its social and medical acceptance well before 1978. On the other hand, although the Western pharmaceutical companies were significantly less successful in the context of Poland’s nationalized industry and state markets, their marketing strategies and persistent attempts to approach Polish institutions throughout the 1960s and 1970s prepared the market for a massive expansion in the 1990s. Dora Vargha (Birkbeck College, UK) discussed the development and coordination of polio live vaccine trials in the late 1950s and early 1960s in as many as fifteen different countries on four continents. Vargha’s presentation revised the common historiographical understanding of the globalization of pharmaceutical research, and demonstrated that the 1950s and 1960s were in fact the crucial decades for the internationalization of drug testing, while polio vaccine trials were among the first truly global phenomena in twentieth-century medicine. Her paper shed light on the nature, assumptions and mechanics of international cooperation between health institutions, governments and individual researchers in organizing polio vaccine trials and evaluating their results. Sarah Hartley (University of York, UK) focused on the international, regional and colonial politics of nutrition in British Colonial Fiji over the two decades after WWII in order to assess how the relationships between various health agencies – UN, WHO and FAO bodies, as well as regional and colonial administrations and offices – affected the design and delivery of nutrition programmes, and the development of international health. Hartley showed how the South Pacific Commission (a Western dominated multi-governmental agency), the South Pacific Health Service (the British and New Zealand colonial health service), and the regional offices of WHO and FAO sought to shape health policy in accordance with their individual ideological and security needs in the South Pacific region. The resulting networks of political and professional allegiance created a patchwork of practice in the field of nutrition across the South Pacific.
In the final analysis, this conference offered a rich and sophisticated account of the complex political and economic circumstances in which twentieth-century international health projects and initiatives emerged and developed – the vagaries of the Cold War constituted the core theme of most presentations. Many papers successfully explored the convoluted relations between pharmaceutical businesses and health organizations; others sought to evaluate the role of experts, their intellectual trajectories and meeting places, as well as their attempts to co-opt political governments for various unorthodox international health endeavours in the context of extreme political rivalries. The conference also emphasized the multiple effects of colonialism and de-colonization on the development of international medicine and health, and several participants attempted to move away from exclusively Anglo-American and Francophone accounts of health globalization. At the same time, while the conference aimed to engage the discussion of scales of historical analysis and to shed light on how international public health programmes were implemented at the local level, it did not devote enough attention to exploring the wealth of social and cultural consequences of such globalizing forces in different parts of the world. Most papers addressed institutional histories or discussed the role and discourses of individual experts, researchers or health administrators, and offered almost exclusively top-down accounts. Many of these narratives would have likely been significantly different – or at least enhanced – if told from the perspective of cultural and social history, history from below and medical anthropology: how did such important international medical and health projects, plans and initiatives transform the social micro-universe of those on the receiving end? did these health programmes induce any significant cultural shifts in how people – patients, physicians, lawmakers – in different parts of the globe thought of and defined illness, death, medicine, political ideology or nation and internationalism? how did the globalization of healthcare and medicine change everyday lives and human interactions? Some of these themes were occasionally touched upon in the course of the conference, but they certainly remain important potential topics for future meetings.
Academic life, as I have learned, makes you painfully aware of the many different regimes of immunization across the globe. Moving between fellowships and jobs, our first son got his vaccines in four different countries – that means four distinct healthcare systems, vaccination schedules, payment structures and vaccination records in three different languages. I think it is safe to say that he has become a reluctant internationalist in his own way. As for us, parents, we pretty much did what we usually do in our working life. We spent hours after each vaccination appointment to analyze the microcosm of public health systems: the doctor-patient encounter. We have been fascinated by the carefully crafted pro-vaccination speech prepared by our American paediatrician, the kind, but firm approach of the German doctors, the inescapable abundance of posters and leaflets on vaccination in the British surgery, and the lack of any kind of publicity and a matter-of-fact discourse in the district paediatrician office in Hungary.
This personal experience has also made me particularly interested in the way childhood immunisation is conceptualised and the points when it is contested or even seems to break down, such as the current ‘anti-vaxx’ controversy prompted by the Disneyland measles outbreak. As I am currently finishing a chapter on debates surrounding the Salk vaccine in Eastern Europe in the 1950s, I started thinking about how communist public health officials would have made sense of debates like this.
An excellent analysis by Jennifer Reich, published in Gender& Society has brought up an important point that would surely have sparked the interest of the communist vaccinators. In this study Reich is speaking to a debate that, in broad brushstrokes, posits crazy and irresponsible people (mainly women) against rational and responsible parents, physicians and public health experts. Reich is arguing that the ‘anti-vaxxers’ are far from being ‘crazy’: in fact, they base their decision on time-consuming research and their choice reflects their social and economic privilege. Not only is this analysis important in understanding current American anti-vaccination movements and their consequences, it also makes clear that behind this potential public health crisis is the primary role of the patient-consumer and an interpretation of personalised medicine. According to Reich’s study, mothers who decided not to vaccinate their children were unconvinced by arguments that they should be participating in public health and expressed that their responsibility was to their own children, not others’. This is along the lines of what popular satirical outlets, such as The Onion have picked up on.
Responsibility for health was exactly the thing in the crux of Cold War attitudes towards public health. Eastern European party dignitaries and public health officials were always happy to boast that countries like Czechoslovakia and Hungary triumphed over polio years before the West and about a decade before the United States did. Their Western colleagues acknowledged the feat, and explained this with totalitarian state organisation – effective epidemic management tends to be authoritarian. The Eastern Europeans had a different explanation, however: the socialist model of organising public health, where prevention is seen as key to the health of the population, healthcare is available to all, vaccines are free, and the paternal state takes responsibility over children’s health. They pointed to the ‘backwardness’ of America for sacrificing the health of children to selfish and market-driven agendas.
Article detailing the Sabin vaccine campaign of December, 1959. Népszava, December 12, 1959. p. 1
Vaccine coverage of course is a marker of superiority only in Cold War rhetoric. It does not reveal much about the quality of healthcare, access to it, or the overall health of a population. Coverage rates can also quickly change due to political unrest and/or economic problems, like in Ukraine, where vaccination has hit critically low rates in the past decade. However, when comparing politically and economically stable countries in the Global North, this difference between East and West does reveal Cold War legacies and attitudes towards the responsibilities of citizens. In much of Eastern Europe, the state expects physicians and parents to comply with vaccination policies without much debate or contestation, and parents expect the state to provide free vaccine and to guarantee its safety. The ‘social’ in medicine is very much still present and high vaccination rates are still a point of pride for Eastern European governments.
Vaccine resistance is also not a new phenomenon. Since there had been vaccines, there has been resistance to it – revealing a wide variety of reasons, usually connected with a much larger issues regarding power relations, distrust, religious integrity, etc. In some societies, like Britain, vaccine resistance has a long history, since the introduction of Jenner’s vaccine.But resistance to vaccines is not even something particularly Western, even if we limit our view to the Global North, although it is slightly more difficult to spot on the Eastern side of the Iron Curtain in the Cold War era. Archival sources give a glimpse of resistance to the Salk vaccine in Hungary, which had to do mostly with opinions that the state was not fulfilling its public health provider role adequately, either by following the ‘wrong’ method of injection, or supplying vaccine lacking in quality and quantity.
There are, of course, new aspects of today’s vaccine resistance in the Global North. Parents have easy access to information online and can establish ties with each other over social media. These ties and the flow of information does not stop at borders, making vaccine resisters at once national agents – in that they respond to a particularly local set of problems of state, public health and culture – and internationalists who participate in shared networks across the globe. Over 25 years after the fall of the Berlin wall, the wind of change might finally reach public health organisation and vaccination in Eastern Europe. In Hungary, where vaccination is compulsory and free, the voice of vaccine critics seems to be growing steadily, drawing mostly on social media, supported by arguments based on translations from English language materials. With a healthcare system that perpetually seems to be on the verge of breakdown – another Cold War legacy -, questions of responsibility for health keep bubbling up to the surface. But for now, the legacy of a previous century is imprinted on my child’s body, who has moved with ease back and forth between East and West, unknowingly becoming a vaccine cosmopolitan.
The New Yorker magazine recently published a piece, titled “The political fight against polio”. This article, reviewing current challenges in polio eradication in Nigeria and conflict ridden areas in general, argues that the polio prevention “plot [got] messy” and has become at least as much of a political, as an epidemiological issue because of its geography. But has polio ever been anything but political? And has it always been a fight?
Polio is a relatively new disease. It started to appear in epidemic waves in the late 19th and early 20th century, and by the 1950s it became a global issue. By then, the epidemic waves became more and more severe and vaccine development saw funding and international cooperation as never before. The stakes were high: this disease spared no-one, it affected rich and poor all the same. Most importantly, polio was (and is) primarily a childhood disease, hence its older name, infant paralysis – a name that is still the official term used in a number of languages. It’s a disease that can cause permanent paralysis, most often in the limbs and occasionally in the respiratory muscles.
Polio’s threat of debilitating future generations was most acutely felt in post-war societies, especially those that suffered a significant blow to their population in World War II. In countries scrambling out of destruction, bracing themselves for a new, albeit Cold War, polio decidedly became political as well as a fight. It is this, post-war setting that ultimately set the tone for the last 60 years of polio. The prevention of contagious diseases became proxy-wars in the Cold War, as in the case of malaria, as Marcos Cueto’s and Randall Packard’s work show. Polio treatment also became a “fight”, whether, as David Serlin points out, encapsulating ideas of heroic masculinity in the West, or as a struggle with the state and its ideologies in the East.
Political agendas have also been ever-present in preventing and treating the disease. These politics are, on the one hand, part of broader perceptions of disease and vaccination, and on the other, are particular to polio. Susan Sontag’s and Emily Martin’s work on AIDS show how contagious diseases are inseparably intertwined with politics. This is, of course, nothing new, Foucault would tell us, pointing to the plague. Even on the level of international disease control, the politics have long played the leading role, as João Rangel de Almeida demonstrates in his research on 19th century efforts.
Perhaps one of the most interesting aspect of the political in the case of polio is its perception as being non-political. In some ways similarly to the smallpox eradication campaign, as Erez Manela’s research shows, conflicting sides made an effort to cooperate in global campaigns of disease prevention. While this seemingly apolitical enterprise was, of course, heavily laden with Cold War politics, it brought together scientists, diplomats and public health officials from both sides in meaningful ways. The intense decade of polio research shows us a different face of the Cold war, and, not in the least, the effort did curb the disease on a global scale. As importantly, in the course of polio vaccine development, key players emerged as guarantors of the “apolitical”: the WHO became a major mediator between East and West when it came to the evaluation of the Sabin vaccine based on Soviet results. With this, the agency was making a strong statement against something the Soviets knew all too well: they were the first to demonstrate the importance of politics in the international organization, when they left it on political grounds shortly after it came to life.
The global “fight” against polio therefore has been represented, and, genuinely perceived by many as being apolitical. That this view is not universally shared, though, should not come as a surprise. While many of the issues that contribute to the challenges of today’s eradication efforts are complex with backgrounds of a wide variety, the history of the disease tells us that fears of polio vaccination and reservations about the international agencies behind it are hardly new. But then, this same history also shows that solutions to polio prevention have cropped up in unexpected spaces, and the last 60 years have resulted in a tangible result: that for millions, polio has become a distant memory.
In November 2013, possibly the largest mass grave from the recent Bosnian war was discovered in the village of Tomasica in the vicinity of the East Bosnian city Prijedor – over 470 bodies of Bosniaks and Croats killed by the Serbian forces have been excavated so far, and the excavations are continuing. It is now estimated that the grave contains between 700 and 1000 bodies. The discovery of the Tomasica grave, in a country where over 8000 people are still missing and many war-related issues remain painfully unresolved, provoked a potent reaction of horror, grief, and anger; it forced thousands to re-live their wartime experiences, loss of family members, memories of mass murders and tortures conducted in eastern Bosnia in the early 1990s. In a divided country, the Tomasica events once again brought to the fore the silence of the Serbian political structures on the issue of war crimes, and directed the public’s attention to the numerous problems in the recent functioning of the UN’s ICTY [International Criminal Tribunal for Former Yugoslavia] in The Hague (which, in 2013, marked twenty years since its foundation in). But Tomasica, quickly becoming a most powerful symbol for the trauma of the Bosnian war, has also been symptomatic of the persistence of mental suffering in the war’s aftermath: the person who led the International Commission of Missing Persons investigators to the site of the grave was a Serbian witness – an army conscript ordered to unload dead bodies into the grave from a truck in 1992. He reportedly testified that he could not bear to fight his own demons any further, that he had been seeing a killed Bosnian man’s open eyes following him everywhere, and that his testimony brought him relief. How have the Bosnian and other former Yugoslav societies dealt with psychological traumatization caused by the 1990s wars? How has war trauma shaped the development of those societies in the aftermath of the conflicts?
From the beginning, the Bosnian war has been coached in clear psychiatric terminology. The ideological explanations of the outbreak of the war were tightly related to the discourse of psychiatry and psychoanalysis, and, at the beginning of the conflicts, the central role was played by psychiatrist politicians and their references to trauma and insanity. Serb war politics in both Croatia and Bosnia-Herzegovina was designed by a prominent psychiatrist of Freudian orientation turned Croat Serb leader Dr. Jovan Raskovic and his protégé in Sarajevo Dr. Radovan Karadzic. It was within a decidedly psychiatric and psychoanalytic discourse that both Raskovic and Karadzic conceived of their respective political roles. Both attempted to introduce madness and trauma as central political categories, with the result that post-Communist politics in Yugoslavia became defined as a form of ‘mass psychiatry.’ In Raskovic’s view, ‘For the Serb, the unconscious desire for nation is paramount and has been suppressed by the ideology of class consciousness;’ post-Communist politics thus needed to forge a proper ‘path to the Serbian Oedipal emancipation.’ A proper psychiatric political leadership was thus critical for the success of this project of political transition and national liberation. Within such a carefully crafted medical discourse, even a planned and coordinated act of genocide could be interpreted as the final expression of ‘healthy madness,’ an irrational delirium which emancipated the nation from its own archaic, primitive Other – the Ottoman legacy, the Muslim presence – and set it firmly on the road to modernity and healthy nationalism.
In a very different context, the psychiatric language has persisted well after the war’s end: the interpretations of the conflict and its aftermath still revolve around the theme of open wounds and psychological re-traumatization. The universality of psychological discourse about the Bosnian war has indeed been one of its most striking characteristics: almost every war crimes-related legal decision in both local and international courts tended to provoke a psychologically-termed response from different victims’ groups. The recent acquittals of high-ranking Serbian and Croatian military and political functionaries at The Hague Tribunal led to a number of negative reactions, especially from Bosniak associations, who reported their loss of faith in the tribunal and considered its decisions an insult to their traumatic experiences. The November 2013 decisions of the European Human Rights Court in Strasbourg and the Constitutional Court of Bosnia-Herzegovina to release ten Bosnian Serb war crime convicts – six of whom were accused of participation in the Srebrenica genocide – due to a procedural issue and re-try them, further reinforced the negative atmosphere among survivors: Munira Subasic, who lost twenty-two male family members in Srebrenica, said that she felt victimized all over again, and that the criminals ‘could even be standing behind [her] back.’
The memorial in Srebrenica (source: thetimes.co.uk)
However, in spite of the potency of such language of psychiatry, the post-Yugoslav states have consistently demonstrated their disregard for the actual psychological problems of their populations. In the aftermath of such a brutal war which primarily targeted civilians, psychological traumatization has remained the subject of non-governmental organizations or autonomous victims’ associations and mainly depended on personal initiative, while no organized or systematic state medical assistance was ever implemented; as a result, a great majority never received any psychological help whatsoever. No meaningful policy for dealing with the war trauma was ever formulated, and masses of traumatized citizens were rarely offered any help in dealing with their persisting mental issues – other than the diagnosis of PTSD and meagre financial aid in the case of certain groups of military veterans.
Part of the reason has been, of course, that the wartime destruction has left these states economically impoverished, with state medical services shrinking, of low quality and increasingly corrupt (particularly in Bosnia, whose complex institutions are often paralyzed as a result of manipulations of ethnic politics). But perhaps even more importantly, the countries most deeply involved in the conflicts of the 1990s – Bosnia and Serbia – have failed, for a number of structural reasons, to integrate the memory of the war into their post-conflict self-image and identity narratives. As a consequence, no stable politics towards understanding and treating the 1990s war trauma has emerged: medical interpretations of war-related mental wounds exist in specific social and cultural contexts and tend to be determined by the collective memory of the conflicts in question, reflected through a collective understanding of the place of those conflicts in the society’s history.
Psychiatric and psychological definitions of war trauma in any particular society tend to reflect the dominant socio-political narrative, and are symptomatic of the most pressing problems the society is dealing with. Dealing with psychological traumatization after war involves attempts to fit potential solutions to lingering problems within the dominant narrative. Twentieth century war psychiatry has proven this numerous times, not least in Yugoslavia itself. For example, in the aftermath of WWII, when various Yugoslav populations were dealing with different forms of profound psychological traumatisation, it was soldiers’ trauma that attracted the state’s undivided attention and became the symbol of wartime psychological suffering. What became known as ‘partisan hysteria’ or ‘partisan neurosis’ was a complicated and apparently unique psychiatric condition, which, according to leading Yugoslav psychiatrists of the era, only affected the victorious soldiers of the Communist resistance movement. While in other combatant countries soldiers’ neurosis mainly comprised anxiety states, shivering or combat fatigue, ‘partisan hysteria’ presented a radically different clinical picture. British, American, Canadian or French soldiers, although on the winning side, suffered from a psychiatric disorder which signified their wish to withdraw from the frontlines, and was symptomatic of their fear of and emotional distance from the battles; by contrast, the Yugoslav partisans’ dedication to the war’s causes was reportedly never compromised, not even when they clearly suffered mental consequences: ‘partisan hysteria’ consisted of epileptiform trance-like seizures, during which soldiers re-enacted their battle experiences, yelled, ‘shot’, ran, even gave political speeches, and thereby expressed their ‘fighting spirit’. Once they recovered from their attacks, the ill partisans would usually not remember anything they did or said during the seizures.
According to Yugoslav psychiatrists and members of the political authorities of the new socialist state, the most striking feature of ‘partisan neurosis’ was that it revolved around this ‘fighting spirit’, the partisans’ continued willingness to fight and re-live battlefield experiences. Instead of being a symptom of fear or exhaustion, it demonstrated the Communists’ continued dedication and courage. The constructed uniqueness of partisan neurosis served very well to underline the uniqueness of Yugoslavia’s postwar political and military position – as a socialist country which bred a large, independent and ultimately victorious Communist resistance guerrilla movement. In many ways, the official interpretation of ‘partisan hysteria’ was an advertisement for Marxist politics and what it could do for the military morale: it created soldiers whose commitment did not falter even when they were facing the worst of their demons. While Western armies conscripted soldiers and forced them to the frontlines to fight for the interests of the capitalist state, the Yugoslav partisans were volunteers in a uniquely egalitarian people’s army and their interests were identical to those of their new socialist homeland.
However, the postwar revolutionary Yugoslav realities were also fraught with a series of problems as reflected in political and psychiatric interpretations and clinical treatment of partisan neurosis. While the ‘partisan hysterics’ were heroes, they also became a symbol of the pitfalls and complexities of an increasingly socially mobile society. One of the most pressing concerns of the postwar period concerned massive social and economic dislocations and elite turnover – this was indeed what made the Yugoslav postwar transformations into a veritable social revolution. But difficulties were still rather formidable, and the Communist Party worried about some of its own members, including those with little education and of peasant origins, and their capacities for contributing their fair share to the revolution. This became particularly important since the new political and military elite was now to be recruited from the ranks of peasants and workers. So it turned out that ‘partisan hysteria’ reportedly only affected partisan soldiers of peasant origin and with little if any formal education – precisely those about whose potential the Party itself was so ambivalent. As psychiatrists and psychoanalysts explained, and the Party tended to agree, it was those undereducated and immature (‘primitive’) young soldiers who simply could not deal with the pressure of their new high-ranking positions, and then broke down, using their neurotic seizures to remind others of their past military achievements and abilities. ‘Partisan hysteria’ was thus portrayed as the pathology of the social revolution. Therefore, the psychiatric understanding of WWII soldiers’ trauma and its treatment reflected the official narrative of the war and resistance, and ‘partisan hysteria’ was seen through the lens of Yugoslav society’s main preoccupation. The concept was a symptom of its time, and its psychiatric and political connotations served socio-political and economic functions in the turbulent postwar times.
However, fifty years later, the political and social situation following the wars of Yugoslav secession was radically different, and the wars’ effects, meanings and interpretations remain far from clear. In Bosnia, the divided state structure prevented the emergence of a unified narrative of the conflict, as different groups and political alliances within the country constantly challenge each other’s interpretation of war events and wartime suffering, while victims’ associations remain in the lurch, manipulated, impoverished, forced to regularly re-live their worst experiences and to prove the authenticity of their pain. Indeed, the post-1995 set-up of Bosnia-Herzegovina did not do much to alleviate the re-traumatizing feelings of injustice: the political leadership of one of the two entities, Republika Srpska, remains stubborn in its chauvinistic rhetoric and refusal to take responsibility for wartime massacres and crimes against humanity, and regularly strives to prevent commemorations of the dead and memorializations of war crimes sites (such as former concentration camps) on its territory (in the most recent example of this trend, Hatidza Mehmedovic, of the association ‘Mothers of Srebrenica’, was summoned to the police of the Serbian entity to make a statement regarding her ‘illegal entrance of private property’ after she went to the agricultural cooperative’s hangar in the village of Kravica to pay respects to over one thousand Bosniak men and boys killed there in 1995). Wartime concentration camp internees can still run into their former guards and interrogators in the streets, because only the highest-ranking perpetrators have ever been legally prosecuted. Hundreds of families have been unable to close the war chapter in their lives because the remains of their missing relatives – children, parents, siblings, spouses – have not yet been found or identified. During the war, the Serbian armed groups conducted a campaign of systematic rape, but this crime remains somewhat of a taboo, even now that rape victims have finally been recognized as civilian war victims, after the 2006 Berlin Golden Bear winner film ‘Grbavica’ by Sarajevo’s Jasmila Zbanic brought the issue to the forefront of the country’s political debate.
A scene from the film ‘Grbavica’, by Jasmila Zbanic (source: worldcinema.org)
In Serbia, war veterans from the recent conflicts face similarly formidable obstacles to reintegration in civilian society and especially to receiving sustained state-sponsored medical and psychological help. In this country, the role of perpetrators and questions about individual and social responsibility for mass war crimes has complicated the process of dealing with the memory of the wars. The Serbian state’s ambivalence about its own role in the 1990s wars has resulted in its failure to address the responsibility issues squarely; instead, the country’s governments have continuously chosen to distance themselves from past military involvements and human rights violations, and focus on the (rather uncertain) future of European integration. But this does not only harm the country’s relations with the rest of the region but also leaves former Serbian soldiers in the lurch. Many of the veterans who are now in dire need of psychological assistance have been struggling unsuccessfully with what they saw and did in Bosnia, Kosovo and Croatia, as well as with developing a stable self-image. How do perpetrators mourn their losses and suffering, and how does a society come to terms with its own citizens whose war participation has been marred by mass war crimes? According to her recent PhD dissertation on Serbian war veterans with PTSD, Belgrade clinical psychologist Olivera Markovic noted that the majority were extremely dissatisfied with their current social and economic position, and resented the state’s neglectful treatment of them as a group (as one of her interviewees said, ‘I defended my country as a patriot and became war invalid, but now I see that this is of nobody’s concern …’). The core problem, in Markovic’s opinion, is that their own relationship to their war activities has become deeply ambivalent, due to the Serbian society’s negative evaluation of the wars of Yugoslav secession, and in particular of the wars’ achievements. This in turn shaped the veterans’ perception that their suffering was in vain, which was reinforced by the state’s sustained neglect of their needs or indeed of their existence. In the absence of any sustained official attempt to come to terms with the wars, war veterans have largely remained unable to make much sense of their involvement in the conflict and of their role in postwar society. Quite ironically, it is one of the most staunchly anti-war non-governmental organizations in Belgrade that developed the only meaningful program aimed at war veterans, and helping them deal with their own psychological issues.
The treatment of ‘partisan hysteria’ in the 1940s Yugoslavia demonstrates the extent to which perceptions of and programs for psychiatric treatment of war trauma depend on the political understanding of wars. In the twentieth century’s culture of universal psychologizing of society and the self, memories of wars tended to be formulated and reinterpreted through the lens of psychological trauma, so that perceptions and the fate of traumatized war veterans or civilians were tightly related to their societies’ collective understanding of the conflicts in question. What happens, though, when the war, which has left hundreds of thousands of victims with severe psychological wounds, has no place in the official memory? Or when, as in Bosnia, over twenty years after it started, the war hasn’t quite ended for so many of its victims? The close relationship between historical memory and treatment of psychological trauma helps to explain the official disregard of mass psychological suffering in the aftermath of the Yugoslav wars in the 1990s. Neither Serbia nor Bosnia has created a stable and coherent political framework for understanding the war, which would make it possible to integrate the issue of war trauma and psychological victimization in the life of the two societies. Certainly, the example of ‘partisan hysteria’ is not one to be followed, but it nevertheless shows that society’s relevance for providing psychiatric and psychological help to war victims and veterans can be intensive and sustained. Maybe there is a way to avoid the overtly political implications of such involvement, and to change the relationship between the politics of memory and the politics of war trauma treatment. It would have to result in the provision of meaningful and considerate psychological assistance to troubled individuals, which would also equip them to become fully-fledged democratic citizens and gain their voice in public discussions of the wars, and it might help these societies overcome their own collective traumas, confusions and denials. This might happen through activities of both the states and a variety of NGOs active in the field of psychology or war memorialization. In this way, re-thinking the meaning and implications of the 1990s war trauma on an individual level could eventually re-shape the collective understanding of the war in a more constructive way.
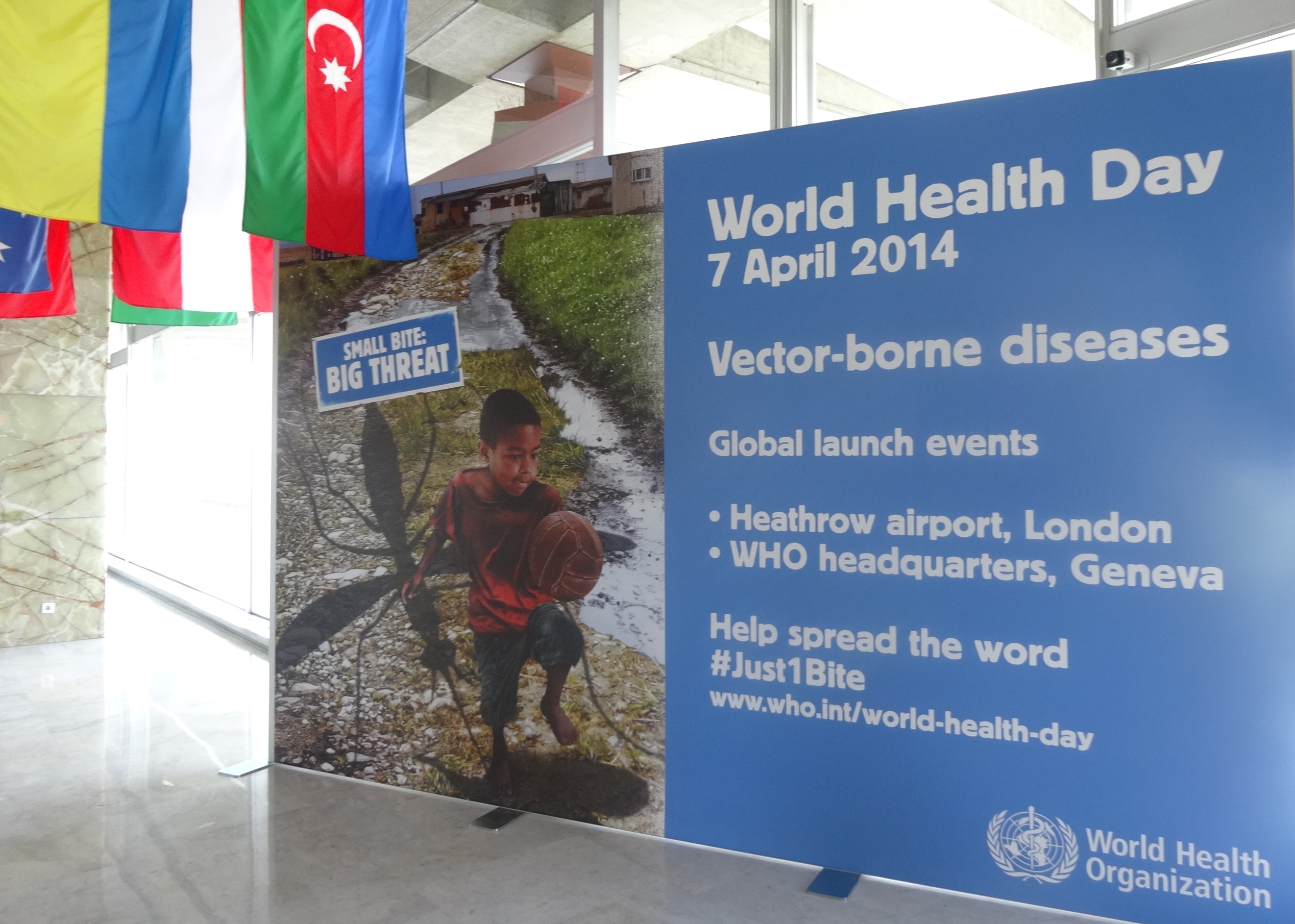
The 65th annual celebration of World Health Day took place last week on 7th April, with a global launch of the Small Bite: Big Threatcampaign against vector-borne diseases at the WHO’s Geneva headquarters. Over half of the global population is at risk of diseases such as malaria, dengue and yellow fever, all of which are preventable but which but have the biggest impact on some of the world’s poorest people. To highlight the risks to travellers, WHO staff installed a 3-D illustration of a giant mosquito at Heathrow Airport and distributed World Health Day boarding passes to passengers, drawing attention to the danger of vector-borne diseases and the simple measures they can take to protect themselves.
‘World Health Days’, the WHO’s Director-General Margaret Chan told visitors to the launch event in Geneva, ‘provide an opportunity to focus world attention on a health problem or issue that deserves special attention.’ Celebrations over recent years have focussed on antimicrobial resistance, climate change and road safety among other issues.
The first World Health Day took place in 1949, not on 7th April but instead on 22nd July, the date that 61 nations had signed the charter of the World Health Organization at New York in 1946. Documents in the WHO archives suggest that the goal of these early events was less to raise awareness of specific health issues, and more, in the words of the first Director-General Brock Chisholm, ‘to encourage public interest in and support of the aims of the Organization.’[1]
In 1949, individual governments were charged with organising events in their own countries and they took up the challenge with varying degrees of zeal. New Zealand led the way with a range of national and local events organized by branches of its United Nations Association. Ireland, Turkey, Austria, Italy and South Africa also responded, organising radio and cinema broadcasts, concerts, press releases and government-directed bible readings amongst other activities. The WHO headquarters in Geneva provided information about the organisation’s early success in combatting malaria in Italy and Greece, providing tuberculosis vaccines in India and responding to a typhus epidemic in Afghanistan. It also distributed a range of publicity materials and suggestions to national government, including a call to issue commemorative postage stamps (a perennial favourite of international organisations at the time).
Not everyone greeted the event with such enthusiasm however. Some countries felt they hadn’t had enough time to prepare suitable activities, whilst others sensibly pointed out that holding such a celebration when most children were on school holidays would severely blunt its impact. The WHO agreed, and the Second World Health Assembly decided that from 1950 World Health Day would be celebrated on April 7th, to commemorate the date in 1948 when the WHO constitution had officially come in to force.
The decision to link World Health Day to the foundation of the WHO highlights some interesting tensions in the early history of the organisation. In 1949 the US and Venezuela protested that they had been successfully celebrating Pan-American Health Day on 2nd December ever since the foundation of the Pan-American Sanitary Bureau (PASB) in 1902, both suggesting that World Health Day should share the same date. The relationship between the PASB and the WHO was one of the biggest areas of debate at the 1946 New York conference that drew up the WHO constitution. Whilst many delegates, particularly from Europe, emphasised the importance of having a single global health organisation, American states were keen to see the work of the PASB continue. The debate around the issue created significant divisions within the conference, including between Britain and the US. Eventually it was agreed that the PASB would continue as the WHO’s regional office for the American continent, although the exact timescale for its incorporation was left deliberately vague.
Implicit in the connection between World Health Day and the foundation of the WHO was the idea that action in the realm of global health somehow began when the organisation was founded, potentially underestimating the legacy of the various international health bodies such as the PASB which had preceded it. To mark this year’s World Health Day, the in-house magazine for the WHO and the UN in Geneva, UN Special, published an article on the birth of the WHO. It focusses on the meeting between three medical men, Szeming Sze, Geraldo de Paula Souza and Karl Evang, at the United Nations Conference on International Organization in San Francisco in 1945. It quotes Szeming Sze’s memoirs as saying the formation of the WHO “all came about quite accidently”, with the first mention of a new health organisation at the conference coming from Dr. Evang at a lunch meeting between the three men, and that it was their efforts to persuade other delegates that led to the decision to create a world health body.
Microfiche copy from the WHO archives of an early WHO document written on an old League of Nations template
Whilst this account is perfectly accurate, it somewhat downplays the extensive debates that had been taking place for at least the previous three years about the design and role of a future international health body, both within Allied governments and international organisations such as UNRRA. Central to these debates was the example of the League of Nations Health Organization, a body which had made significant contributions to the field of international health in the interwar period and which ultimately provided much of the template for the design of the WHO. It had continued to function in a much reduced form throughout the Second World War and its leading members were active participants in the debate about the shape of a post-war world health body. When the WHO Interim Commission began its work in 1947, it based itself in the same building as the League’s health section, employed many of the same personnel, and as we can see from the document above, even used the same stationery.
Indeed the same vector-borne diseases that the WHO was and is working to combat were also a key focus for the League, which established its own malaria commission in the 1920s. The fact that after nearly a century of international activity these diseases remain such a problem highlights the relevance of this year’s World Health Day campaign.
Further Reading:
Yves Beigbeder et al., The World Health Organization (Dordrecht: Nijhoff, 1998)
Iris Borowy, Coming to Terms with World Health: The League of Nations Health Organisation 1921-1946 (Berlin: Peter Lang, 2009)
Neville Goodman, International Organizations and Their Work (Edinburgh: Churchill Livingston, 1952)
Szeming Sze, The Origins of the World Health Organization: A Personal Memoir 1945-1948 (Boca Raton: L.I.S.Z. Publications, 1982)
Paul Weindling (ed.), International Health Organisations and Movements, 1918-1939 (Cambridge: Cambridge University Press, 1995)
[1] Documents relating to the history of World Health Day can be found in the WHO archives, Centralized Files First Generation, section 400-1-2. All unattributed material from this post comes from these files.
Patients on their way to the Matsesta baths from the Sanatorium Krasnaia Moskva in 1928 or 1929. From Sochi: Stranitsy proshlogo i nastoiashchego, ed. A.V. Guseva (Sochi: Muzei istorii goroda-kurorta Sochi, 2007).
The Olympic website for Sochi 2014 (http://torchrelay.sochi2014.com/en/city-sochi) and media coverage occasionally detail the history of the development of Sochi, tying it in the main to the growing popularity of sea bathing in Russia in the early twentieth century. The rise of sea bathing certainly did increase the popularity of the resort, in the context of the rise of tourism on the entire Black Sea coast. But that is only part of the story. The resort was also developed, after the discovery of the presence in Sochi of sulpheric mineral waters at the source “Matsesta,” as a resort for mineral water cures. Many of the first tourists to Sochi were actually patients.
While “taking the waters” is unfamiliar to many people, it was at the time of the first and second waves of development in Sochi – in the 1910s and mid-1930s – still mainstream medical therapy throughout Europe, and continues to be in many places to this day. The mid- to late-nineteenth century saw the rise of the baths, tied to the spread of the railways and increasing accessibility of travel to an expanding bourgeoisie. The circulation of visitors to baths in Central Europe increased dramatically in the 1850s, in the wake of railway construction. The leading baths of Central Europe were Wiesbaden and Baden-Baden, which saw about 30,000 visitors a year each in the 1850s. In Imperial Russia, the railway reached from Rostov-na-Donu to the Caucasian Mineral Waters, an established military resort, in 1875, leading to a burst in the construction of hotels, dachas (summer cottages) and restaurants. That decade the railways also reached the baths of the Austro-Hungarian Empire. In 1888, the railway reached the Black Sea port of Novorossiisk, opening the Black Sea coast of the Caucasus, where Sochi is located, to a new wave of development. As the railways reached out into the flesh of the empires, circulation began to flow domestically and internationally.
As today, the development of the Black Sea coast was spurred by state intervention and investment. The region was in the early twentieth century scarcely populated, and attempts to settle peasants from other places in the empire there as farmers, through various economic and social incentives, were not a success. A particular problem was that malaria was endemic to the region. In the late nineteenth century, Tsar Nicholas II began to ponder targeting the coastline as a site for the development of tourism. But what would draw people to the region?
In 1912, the Tsar sent a large delegation of scientists, including the leading balneologists of the empire, to the region to search for mineral water sources. If mineral waters could be found, perhaps they could serve as a nucleus to draw tourists to the region (and away from rival baths in Central Europe). The delegation reported back that their greatest hopes had been answered. The region was laden with rich deposits of mineral waters, largely untapped. The scientists compared the baths of Matsesta to the baths of Aachen in Western Germany, due to their sulpheric content, a mineral water source called the Kaiserquelle.
The news of the riches of the region, and imperial approval for their development, spread quickly. The first development of the Matsesta waters rested on private capital. A joint stock company was formed to fund the development of the Matsesta mineral waters and in 1912, the first bath house there was opened. Sochi-Matsesta was an ingénue among resorts – aristocrats largely remained loyal to the more established Crimean resort of Yalta or the Caucasian Mineral Waters resort. The Black Sea Coast was particularly attractive to a middle class health resort patient, or kurortnik, as well as patients of the Jewish faith (whose presence was banned at established Imperial Russian resorts). Dachas and villas as well as modest pensions and inns began to be built and there was even some land speculation. Sochi-Matsesta boomed, very briefly, and the development of spa medicine improved when imperial resorts served the front during World War I. The resorts on the Black Sea coast grew from almost nothing at the beginning of the twentieht century through the help of speculators and developers to receive 75,000 visitors in 1912.
A Patient at the Matsesta bath house in the 1920s. From L.G. Gol’dfail’ and I.D. Iakhnin, Kurorty, Sanatorii i doma otdykha SSSR 1928 (Moskva: Gosudarstvennoe izdatel’stvo, 1928).
With the Bolshevik revolution of 1917, the fate of the resorts of the empire seemed unclear. In the nearby Weimar Republic in Germany, for example, despite revolution, the celebrated baths remained largely in the hands of the elite segments of society, beyond the reach of the state. But the Communist party and state was determined to develop health resorts “for the workers.” In 1919, Lenin signed a decree nationalizing all health resorts, which reserved them for the use of the workers, peasants and Red Army soldiers in first order, for medical treatment. Filling the old Tsarist palaces with workers and peasants had obvious propaganda value. In Sochi, sanatoria were established in pre-revolutionary villas, hotels and private clinics (see Figure 1). But the level of state investment in the network of health resorts, and of medical services there, make it clear that this was not a mere “Potemkin village.” The state, and particularly the committed physicians at the head of the new, state public health ministry, the Commissariat of Public Health, took health resort medicine seriously, not least mineral water treatments, as a way to improve the health of the entire population.
The use of the Matsesta waters increased dramatically, largely due to patients sent for a “cure” by the Commissariat of Public Health (See Figure 2). In the 1920s, a cure usually lasted from four to six weeks, and included from 15 to 30 baths with Matsesta waters. Physicians sent patients to Matsesta to cure chronic eczema and other skin conditions, gout, various nervous ailments, syphilis, chronic rheumatism, gynecological ailments and ailments of the heart, circulation and digestion, but patients also took the waters of their own accord, “off label,” for whatever ailed them. The number of patients using the Matsesta waters increased from 67 in 1920, to 3,921 patients in 1925. The most rapid expansion, however, came during the years of industrialization of the late 1920s and 1930s: from 1927 to 1932 the number of patients taking the Matsesta cure increased from 7,980 patients to 48,574 patients. The number of baths taken increased from 1921 to 1932 from 1,345 baths to 731,218 baths. A second bath house was built. But demand outpaced supply. By 1937, the Matsesta bath houses were working from 6 a.m. until 11 p.m.
The Soviet leaders were justifiably proud of their accomplishment, but rather overstated their role in developing the resort. Frequently not included in Soviet statistics were numbers from the pre-Revolutionary period: 18,604 baths were administered in 1913, 17,395 baths in 1914, 16,982 baths in 1915 and 21,586 baths in 1916. Indeed, the pre-revolutionary peak in 1916 was not reached in the Soviet Union until 1923. In the 1920s and 1930s, as now, the idea that the resort was “new” served the symbolic project of treating their development as a display of state power. Patients continue to take the cure at the Matsesta waters to this day (See Figure 3).
The bath house “Staraia Matsesta” in 2009. Photograph taken by the author
For Further Reading:
Diane P. Koenker, Club Red: Vacation Travel and the Soviet Dream (Ithaca: Cornell University Press, 2013).
Mirjam Zadoff, Next Year in Marienbad: The Lost Worlds of Jewish Spa Culture (Philadelphia: University of Pennsylvania Press, 2012).
Douglas Peter Mackaman, Leisure Settings: Bourgeois Culture, Medicine and the Spa in Modern France (Chicago: Chicago University Press, 1998).
John K. Walton, ed., Mineral Springs Resorts in Global Perspective: Spa Histories (London: Routledge, 2013).
Eric Thomas Jennings, Curing the Colonizers: Hydrotherapy, Climatology and French Colonial Spas (Durham: Duke University Press, 2008).
Dora Vargha’s blog post on November 25th discussed the current financial difficulties faced by the Peto Institute in Budapest in the context of historical approaches to disability in Hungary. The Institute may be familiar to British readers who remember its rise to prominence in the late 1980s and its role in the debate around conductive education in the treatment of children with neurological disorders. The links between the UK and the Peto Institute provide a fascinating example of patient-led transnational history in Cold War Europe.
Princess Diana at the Peto Institute (1990)
The Institute first came to public attention following the broadcast of the BBC documentary Standing up for Joe in April 1986. The documentary followed the story of the Hadley family who had taken their severely disabled son to Budapest for treatment. The Institute pioneered the system of conductive education developed by its founder, Andras Peto, in the aftermath of the Second World War, which involved an intensive programme of physical and speech therapy under the supervision of “conductors” combined with very high expectations of the progress children could achieve.
The documentary, broadcast at prime time on BBC1 and watched by over five million people, caused a national stir. The BBC received 11,000 letters of enquiry, questions were asked in parliament, and a lobby group, the Foundation for Conductive Education, was set up to promote its use in the UK. The system was presented in the media as more holistic than the medicalised approach to treatment in the UK, and many parents were attracted by the positive expectations it had of potential progress against a perceived negativity and conservatism amongst UK medical staff. Over the following years UK families flocked to Budapest, often supported by national and local campaigns to raise funds for treatment. The Times estimated that over 600 UK children had visited the centre by 1990.
However, the treatment was not without controversy. Many within the British medical establishment felt that the claims for its success were overblown, and that the appearance of progress owed much to the fact that the Institute was selective in the cases it accepted. The Chartered Society of Physiotherapy published a report in 1988 questioning many of the Institute’s claims, whilst the Spastics Society, initially wary of the programme, was picketed by the Foundation for Conductive Education over claims that its own conductive education schemes weren’t the real thing.
One of the most interesting features of the coverage of the Institute is its presentation in the context of the Cold War. Andrew Sutton, the Director for the Foundation for Conductive Education, described it as a ‘Len Deighton Cold War story, coming from a street near you’, with the media frequently describing families moving “beyond the iron curtain”. It certainly represents one of the most widespread and high profile instances of UK residents experiencing life in the Eastern Bloc prior to the end of communism. The BBC’s follow-up documentary to Standing up for Joe broadcast in 1987, which tracked the story of the British families who had followed in the Hadley’s footsteps, was entitled To Hungary with Love.
The Peto Institute also played a role in Anglo-Hungarian relations during the transition to democracy. In December 1989 the UK government announced £5 million of funding for the Institute’s new international centre to guarantee places for British children and pay for training of a group of British conductors. This funding was discussed as part of a wider package of support when Hungarian Prime Minister Miklos Nemeth visited Margaret Thatcher on December 14th. In an article on the 6th January, The Times presented the funding as part of a range of government measures to form closer medical and scientific links with the Soviet Union and Eastern Bloc countries. Following the first free elections in March 1990, Princess Diana made a high profile visit to the Institute as part of a four-day tour of Hungary where she presented an honorary OBE to its director, Dr Maria Hari.
The controversy around conductive education has never entirely gone away. In 1993 the government-commissioned Birmingham Project indicated that it was no more effective than comparable UK treatments, a claim that continues to be challenged by its adherents, whilst in 2003 Peter Randall from Kent attempted to sell his kidney on ebay to fund conductive education for his daughter. Although conductive education is now more widely available in the UK, British children continue to visit to Peto Institute for treatment.
When we started to think about ways to visually present the concept of internationalism for the purposes of our research project, we faced a number of difficulties. What do we mean by ‘internationalism’, and who is the most appropriate to represent it? What exactly does ‘internationalism’ do?
In order to resolve these questions, we realised that we must first understand and contextualise the multiplicity of meanings assigned to the concept. In historiographical literature, we have regularly come across the assumption that internationalism is bound to represent a force of good, a benevolent process predicated on humanitarian assumptions, and meant to increase mutual understanding and respect between nations. However, such scholarly readings seem to omit a very important point: in the course of the nineteenth and twentieth centuries in particular, internationalism came to denote a number of different and often unrelated processes and efforts which included governments, non-governmental institutions, politicians, experts of all kinds, refugees and stateless people, etc. Moreover, internationalism appeared in a number of different guises, and proclaimed radically different ideological, social and political aims and goals, some of which were indeed far from humanitarian, democratic or cosmopolitan. Even more importantly, internationalism was perceived in a variety of ways by different audiences. And while the globe of the world seems to be rather popular as a positive symbol of internationalism, a number of scholars dealing with the history of this phenomenon have often tended to overlook the globe’s cynical or sardonic uses (and their broader implications). Such uses, though, have been equally important for articulating critical appraisals of some particularly negative effects of certain forms of internationalism. It is, therefore, our aim to explore alternative visualisations of internationalism, and to use them as a tool for understanding and historicising radically different visions and interpretations of this concept.
Figure 1 (Source: Bowman Gray Collection of World Wars I and II, Rare Book Collection, Wilson Library, University of North Carolina Chapel Hill)
It was in the course of WWI that different visions of the international order clashed causing a veritable global explosion, while the orgy of what came to be seen as purposeless violence and chauvinism provoked disappointment in the ranks of those who hoped that a more tightly interconnected world would lead to more stable peace. Interestingly, while WWI marked the failure of nineteenth-century liberal internationalism, it was also the origin of a new and highly ambitious concept of ordering international relations. In a series of Italian postcards from WWI, several cartoonists and painters, such as R. Ventura and Aurelio Bertiglia, articulated this profound disappointment with some of the predominant agents of internationalism at the time, and used the image of the globe in imaginative, sarcastic and unusual ways in order to reinforce their political message.
These postcards were an essential part of WWI political propaganda, and contributed to the extremely extensive propaganda campaigns undertaken by the Entente governments to discredit German military conduct and involvement. One of the most striking phenomena related to WWI was the importance political governments attached to public mobilization through atrocity reports and similar psychological techniques to demonize the enemy; moreover, from the very beginning of the war, different governments worked to revise or falsify original documents in order to place the blame for the outbreak of WWI on the enemy side, so that historiographical debates regarding the origins of WWI began as early as 1914. In 1918, Germany was forced to accept full responsibility for ‘all the loss and damage’ caused to the Allied countries; however, throughout the conflict, the Allied governments carefully worked toward this placing of the full burden of war guilt on Germany (and her allies). The ‘guilt clause’ was carefully prepared through numerous propaganda campaigns, which depicted Germany in particular as a brutal and even demonic force. It was this strong anti-German sentiment that informed the theme and style of the Italian postcards. The postcards were created in 1915 or 1914, around the time the Italian government negotiated joining the war on the side of the Entente against her former allies in the Triple Alliance – Germany and Austria-Hungary – which explains the political edge of the postcards. As is clear from Figure 1, the postcards also expressed a strong anti-Austrian feeling, which was hardly surprising given Italy’s long-standing territorial pretensions to large parts of the Habsburg Empire.
The first postcard, from about 1914, depicts a ‘bloody handshake’ between the leaders of two Central Powers: Austria-Hungary’s Franz Joseph and Germany’s Wilhelm II. It is captioned ‘The Pact’, and uses the globe to articulate a pithy critique of the German- and Austrian-led attempts at (re-)ordering the international affairs: through their particular vision of internationalism, the Habsburg Emperor and the German Kaiser have plunged the entire world into a bloody conflict. The alliance between the two powers is then held solely responsible for the outbreak of the conflict, and their incompetent leadership as well as the malicious effects of their political friendship are exposed to ridicule and contempt. Yet another postcard, from 1915, communicates a very similar political message, but, in addition, emphasizes the Central Powers’ criminal negligence towards the rest of the world, with which they toyed for their own selfish purposes and self-aggrandizement. In Figure 2, Wilhelm II and Franz Joseph play football with the globe before an assortment of international onlookers. The caption says ‘How small the world is’, and captures perfectly the cartoonist’s message regarding the two leaders’ self-centredness, ignorance and inadequacy.
In a number of postcards, Germany, represented by Wilhelm II, was depicted as extremely militaristic, aggressive, ruthless and greedy for world power. In a series of pictures, Wilhelm II endeavours to take possession of the world in a number of ways. In Figure 3, dressed in a full military uniform and also wearing a helmet, the Kaiser actually reaches to grab the globe, while war and violence rage behind his back. The map of Italy is quite prominent on the globe itself, while the cartoon implies quite forcefully that the conflict was a result of Wilhelm’s obsession with ruling the world. Interestingly, the sun itself is against Germany’s (unnatural?) expansion, and warns the Kaiser in the caption that it will burn his hands.
In Figures 4 and 5, the same interpretation of Germany’s relationship with the rest of the world was expressed, and German militarism and aggression singled out as the primary culprits for the contemporary global catastrophe. In both postcards, Wilhelm II attempts to actually eat the globe. In Figure 4, the caption calls him ‘the glutton’, and he obviously finds his food of choice a bit too hard to crack.
In Figure 5, in which Wilhelm II actually cuts into a watermelon in the shape of the globe, the postcard similarly warns him: ‘Mind you, this might give you indigestion.’ This cartoon further emphasized the supposed bloodthirstiness and criminality of Germany’s wartime conduct and ambitions: on Wilhelm’s table, the globe of the world is accompanied by a baby with French and Belgian flags sticking out of its belly, and a bottle of wine filled with ‘Latin blood.’ The Kaiser’s sword and helmet, the ultimate symbols of his and his country’s aggressive militarism, rest by his feet.
Figure 5 (Source: Bowman Gray Collection of World Wars I and II, Rare Book Collection, Wilson Library, University of North Carolina Chapel Hill)
It was these and similar critiques that aimed to contribute to strengthening public support for the war, and to foster and encourage nationalist, even chauvinistically anti-German and anti-Austrian, sentiments. Quite paradoxically, however, they also provoked a far-reaching rethinking of possibilities, limitations and potential meanings of political internationalism in Europe during and after WWI, and gave an important impetus to implementing a new, more ambitious vision of world governance, which was to be institutionalised and developed in the interwar years. It was in this context of the war, destruction and vicious nationalist propaganda that the project of internationalism was infused with renewed significance, and brought back to the centre of political discussions. These postcards articulated powerful criticisms of Europe’s pre-war alliance system and pointed out its deleterious consequences; their messages were part of a broader movement that emphasised the shortcomings of pre-WWI forms of international cooperation, and encouraged a political and intellectual search for a different postwar order which would ensure permanent peace.
Nothing Found
It seems we can’t find what you’re looking for. Perhaps searching can help.



 Earlier this summer, Birkbeck played host to a two-day conference on the international history of the Spanish Civil War.
Earlier this summer, Birkbeck played host to a two-day conference on the international history of the Spanish Civil War.